

Review
doi: 10.2215/CJN.03170313.
Epub 2014 Jan 23.
Renal relevant radiology: use of ultrasound in kidney disease and nephrology procedures
Affiliations
- PMID: 24458082
- PMCID: PMC3913230
- DOI: 10.2215/CJN.03170313
Item in Clipboard
Review
Renal relevant radiology: use of ultrasound in kidney disease and nephrology procedures
Clin J Am Soc Nephrol.
2014 Feb.
Abstract
Ultrasound is commonly used in nephrology for diagnostic studies of the kidneys and lower urinary tract and to guide percutaneous procedures, such as insertion of hemodialysis catheters and kidney biopsy. Nephrologists must, therefore, have a thorough understanding of renal anatomy and the sonographic appearance of normal kidneys and lower urinary tract, and they must be able to recognize common abnormalities. Proper interpretation requires correlation with the clinical scenario. With the advent of affordable, portable scanners, sonography has become a procedure that can be performed by nephrologists, and both training and certification in renal ultrasonography are available.
Figures
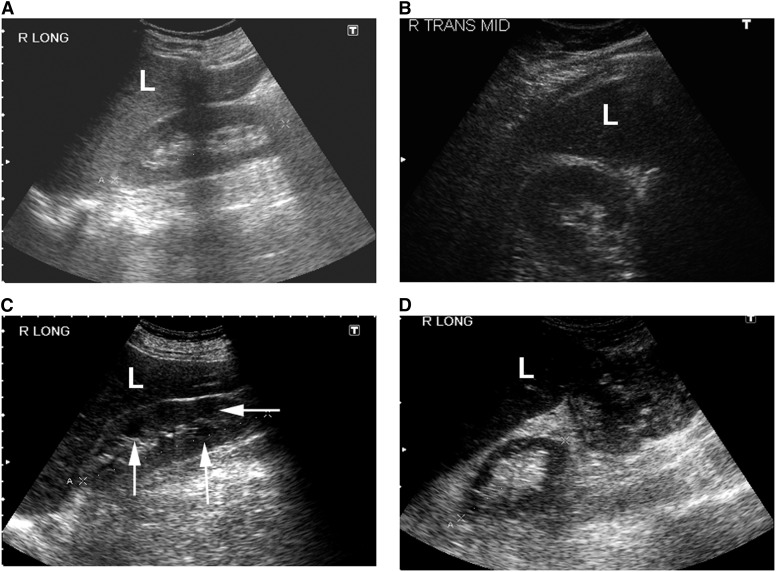
Sonographic appearance of the renal parenchyma. (A) Normal right kidney (longitudinal view). (B) Normal right kidney (transverse view). (C) Echogenic right kidney with prominent medullary pyramids (arrows). (D) Atrophic right kidney (longitudinal view) with thin parenchyma and containing mostly sinus fat. L, liver.
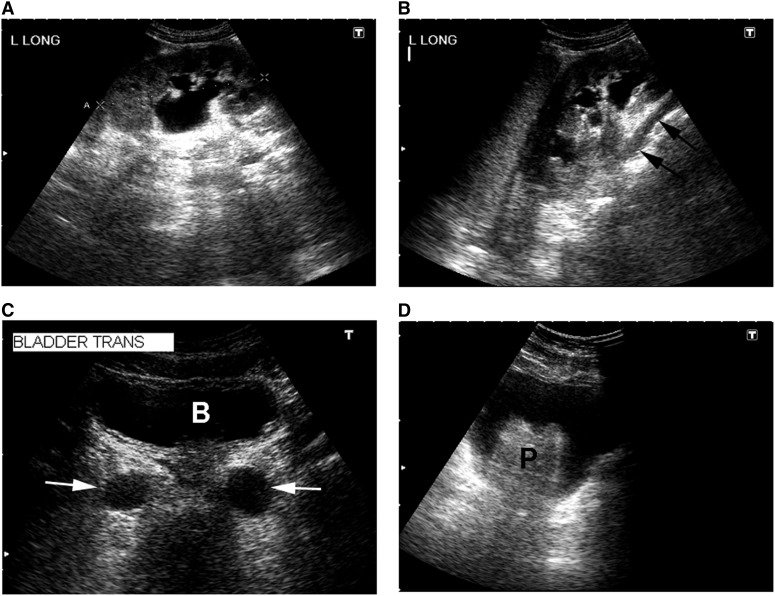
Sonographic appearance of the upper and lower urinary tract. (A) Hydronephrosis of a left kidney (longitudinal view) with dilated renal pelvis and major and minor calyces. (B) Another longitudinal view of the same kidney showing a dilated ureter (arrows) tracking underneath the lower pole. (C) Transverse view of the urinary bladder (B) showing dilated distal ureters (arrows). (D) Transverse view of the urinary bladder with an enlarged prostate gland (P).
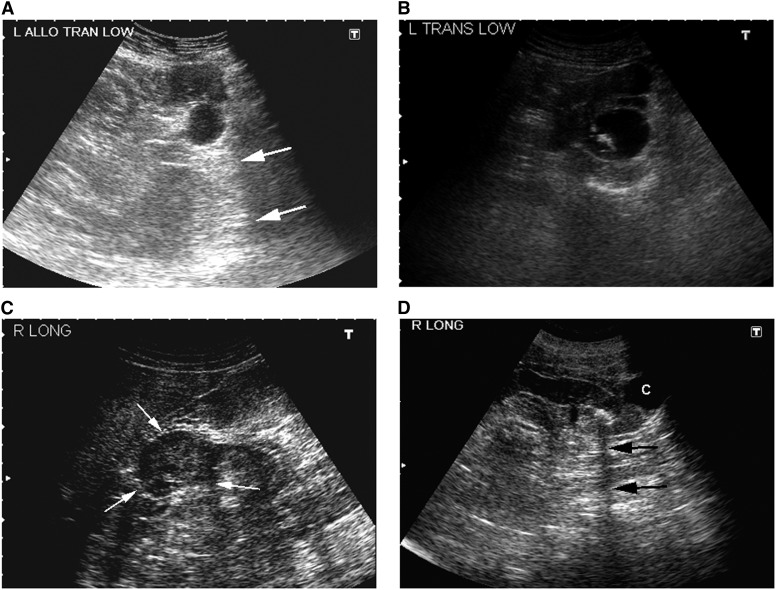
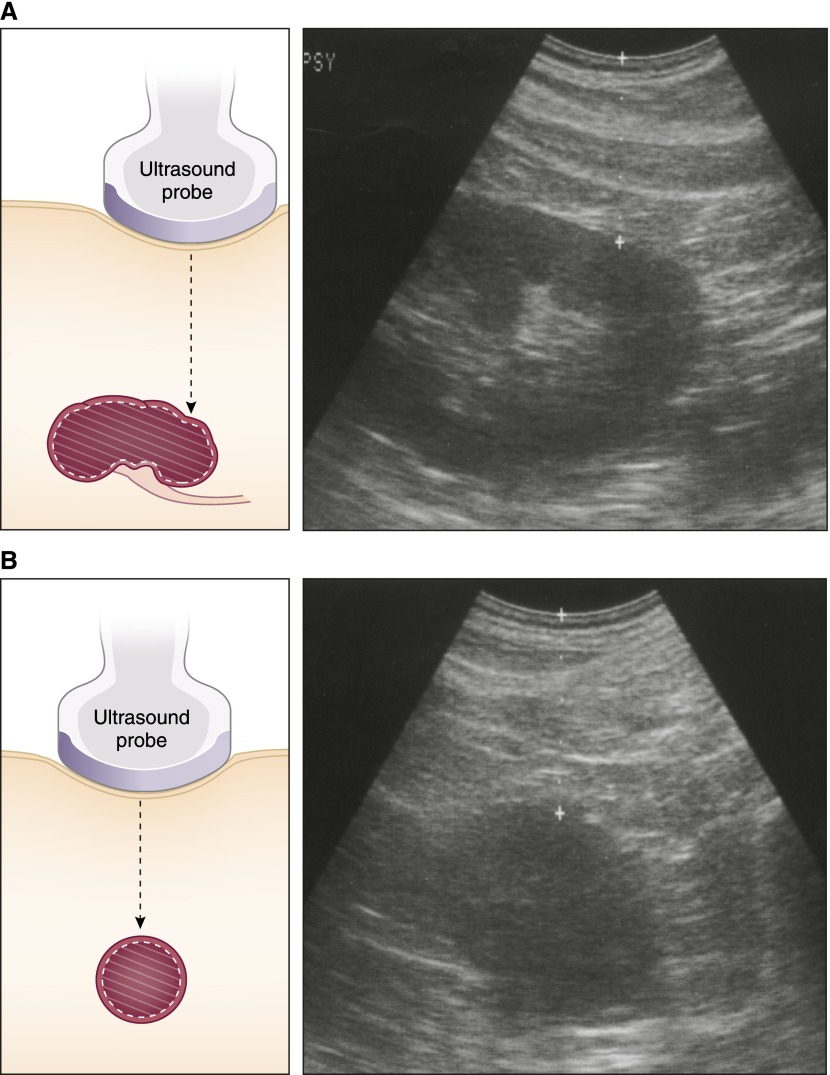
Sonographic appearance of renal masses. (A) Simple cyst in the lower pole of a renal allograft (transverse view). Note the round, smooth, and thin wall and absence of internal echoes. The distal enhancement (arrows) indicates that it is fluid-filled. (B) Complex cyst in the left mid-kidney containing echogenic material (transverse view). (C) Solid mass in the right mid-kidney (longitudinal view). Note the echogenicity within the mass and the lack of distal enhancement. (D) Stone in the lower pole of a left kidney (longitudinal view) casting an acoustic shadow (arrows). There is also a simple cyst (C).
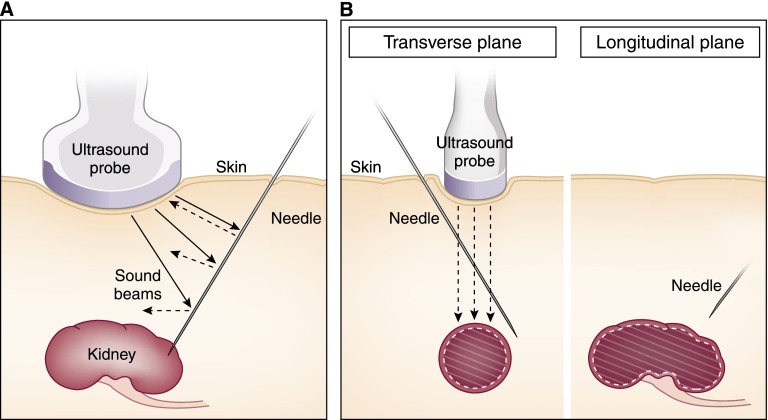
Ultrasound principles of real-time visualization. (A) Needles are specular reflectors from which sounds reflect at the angle of incidence. Only the sound that strikes at a perpendicular angle returns to the probe. Other sounds may not reach the probe and those portions of the needle will not be detected. (B) Needles (left) not maintained within the width of the sound beam will appear shallower than (right) their true depth on the sonogram.
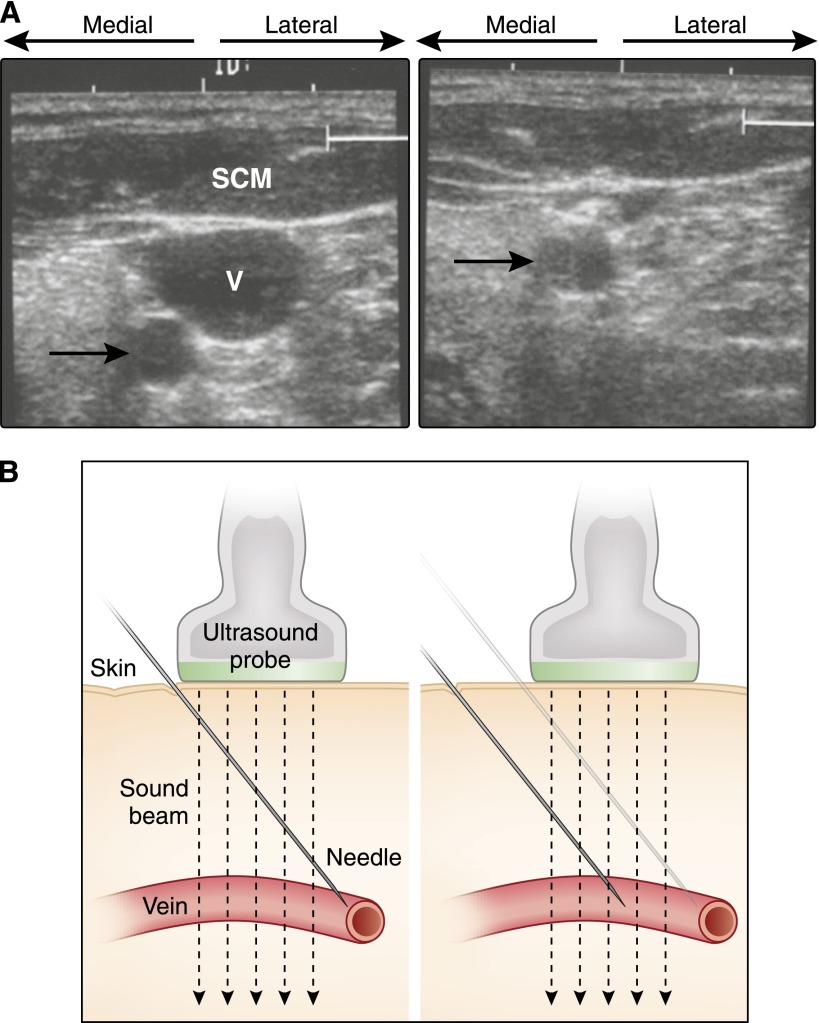
Sonographic guidance of central venous cannulation. (A) Transverse view of the anterior neck. The internal jugular vein (V) is underneath the sternocleidomastoid muscle (SCM). The carotid artery (arrow) is posterior and medial to the vein, and it is positioned outside the path of a needle into the center of the vein. Right panel shows the collapse of the vein, but not the artery, with compression. (B) The needle should be offset from the probe and at an angle such that (right) it enters the vein within the sound beam.
Ultrasound marking for percutaneous renal biopsy. The lower pole is positioned directly under the center of the probe in the (A) longitudinal and (B) transverse planes. Note the absence of sinus fat in the transverse view, indicating that only renal parenchyma will be in the path of the needle.
References
-
- O'Neill W: Atlas of Renal Ultrasonography, Philadelphia, Saunders, 2000
-
- O’Neill WC: Sonographic evaluation of renal failure. Am J Kidney Dis 35: 1021–1038, 2000 - PubMed
-
- O’Neill WC, Baumgarten DA: Ultrasonography in renal transplantation. Am J Kidney Dis 39: 663–678, 2002 - PubMed
-
- O’Neill WC, Bardelli M, Yevzlin AS: Imaging for renovascular disease. Semin Nephrol 31: 272–282, 2011 - PubMed
-
- Bakker J, Olree M, Kaatee R, de Lange EE, Moons KGM, Beutler JJ, Beek FJ: Renal volume measurements: accuracy and repeatability of US compared with that of MR imaging. Radiology 211: 623–628, 1999 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
