

Hypernatemia : successful treatment
- PMID: 24459489
- PMCID: PMC3894528
- DOI: 10.5049/EBP.2006.4.2.66
Hypernatemia : successful treatment
Abstract
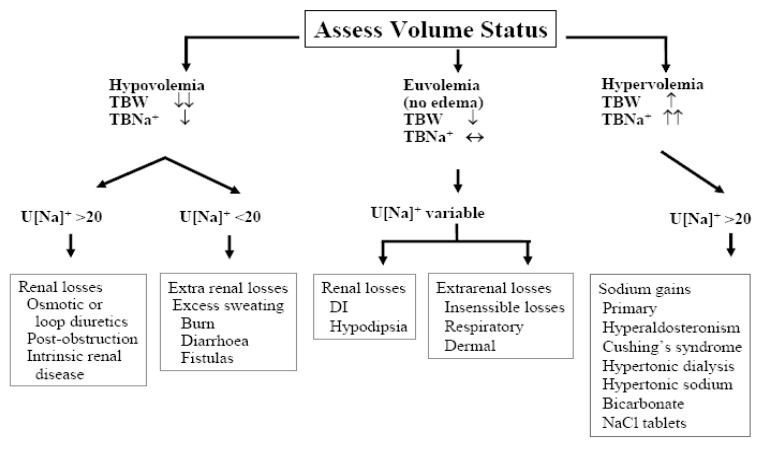
Hypernatremia reflects a net water loss or a hypertonic sodium gain, with inevitable hyperosmolality. Severe symptoms are usually evident only with acute and large increases in plasma sodium concentrations to above 158-160 mmol/l. Importantly, the sensation of intense thirst that protects against severe hypernatremia in health may be absent or reduced in patients with altered mental status or with hypothalamic lesions affecting their sense of thirst and in infants and elderly people. Non-specific symptoms such as anorexia, muscle weakness, restlessness, nausea, and vomiting tend to occur early. More serious signs follow, with altered mental status, lethargy, irritability, stupor, and coma. Acute brain shrinkage can induce vascular rupture, with cerebral bleeding and subarachnoid hemorrhage. However, in the vast majority of cases, the onset of hypertonicity is low enough to allow the brain to adapt and thereby to minimize cerebral dehydration. Organic osmolytes accumulated during the adaptation to hypernatremia are slow to leave the cell during rehydration. Therefore, if the hypernatremia is corrected too rapidly, cerebral edema results as the relatively more hypertonic ICF accumulates water. To be safe, the rate of correction should not exceed 12 mEq/liter/day.
Keywords: Cell volume regulation; Diabetes insipidus; Hypernatremia.
Figures
References
-
- Adrogue HJ, Madias NE. Hypernatremia. New Engl J Med. 2000;342:1493–1499. - PubMed
-
- Petis LD, Luchitti A, Emma F. Cell volume regulation and transport mechanisms across the blood-brain barrier: implications for the management of hypernatremic states. Eur J Pediatrics. 2001;160:71–77. - PubMed
-
- McManus ML, Strange K. Acute volume regulation of brain cells in response to hypertonic challenge. Anesthesiology. 1993;78:1132–1137. - PubMed
-
- McDowell ME, Wolf AV, Steer A. Osmotic volumes of distribution: idiogenic changes in osmotic pressure associated with administration of hypertonic solutions. Am J Physiol. 1955;180:545–558. - PubMed
-
- Strange K. Regulation of solute and water balance and cell volume in the central nervous system. J Am Soc Nephrol. 1992;3:12–27. - PubMed
Publication types
LinkOut - more resources
Full Text Sources