

Electrolyte and Acid-base disturbances associated with non-steroidal anti-inflammatory drugs
- PMID: 24459510
- PMCID: PMC3894511
- DOI: 10.5049/EBP.2007.5.2.116
Electrolyte and Acid-base disturbances associated with non-steroidal anti-inflammatory drugs
Abstract
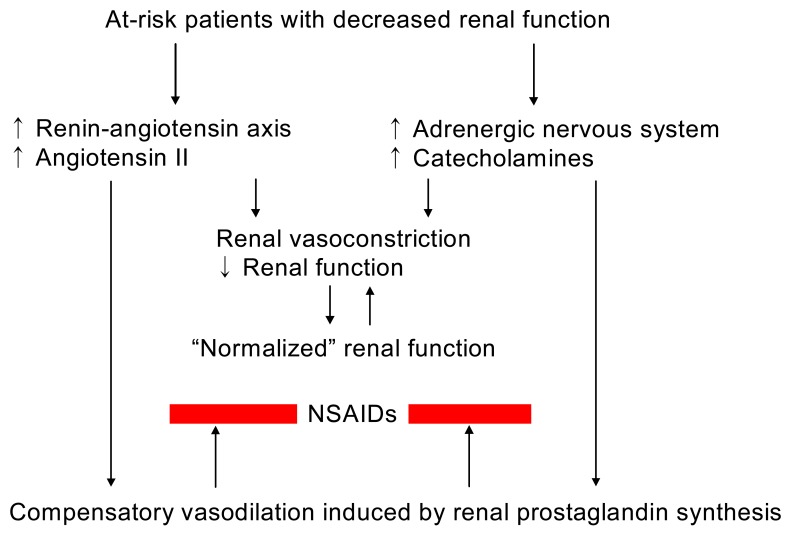
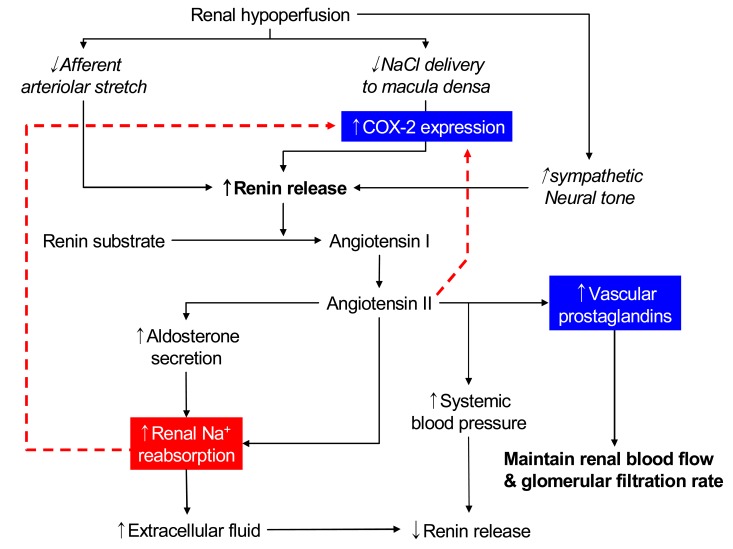
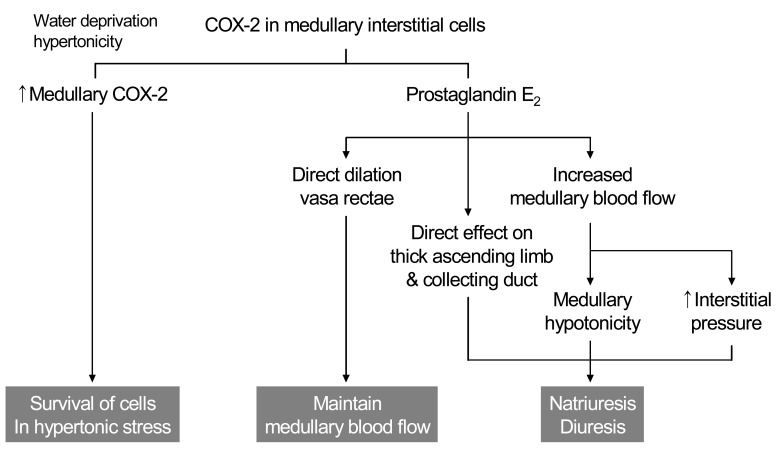
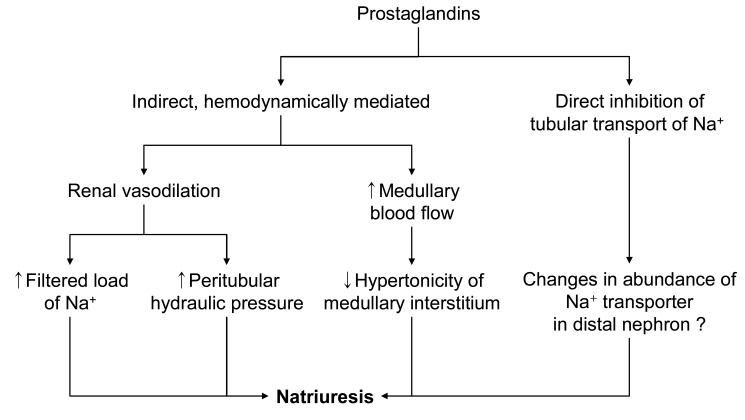
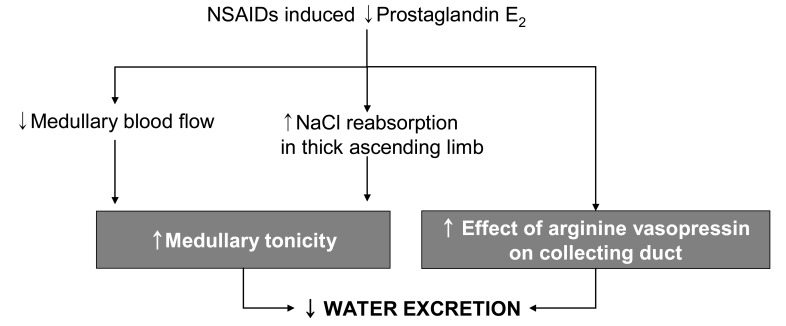
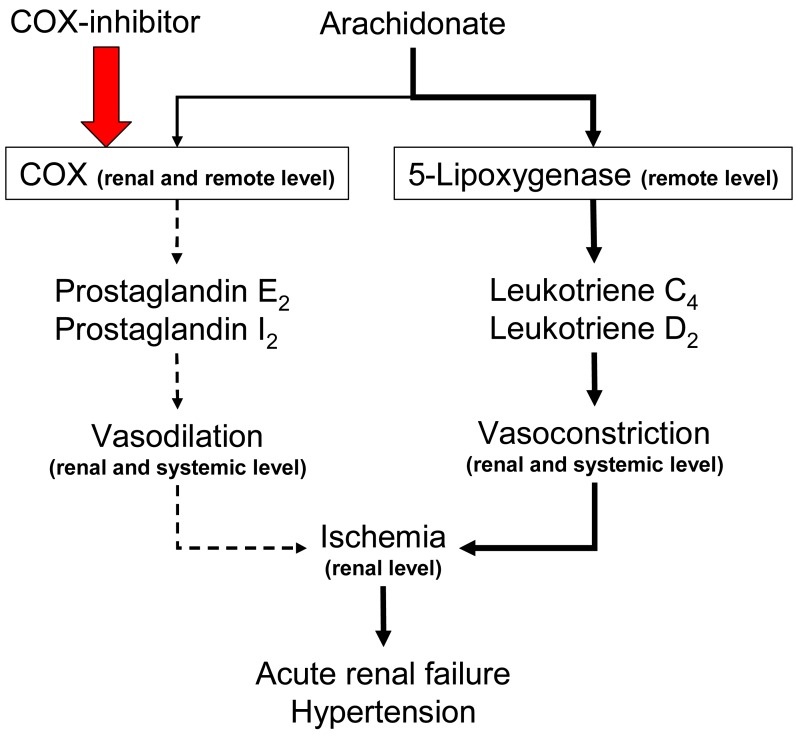
Inhibition of renal prostaglandin synthesis by non-steroidal anti-inflammatory drugs (NSAIDs) causes various electrolyte and acid-base disturbances including sodium retention (edema, hypertension), hyponatremia, hyperkalemia, and decreased renal function. Decreased sodium excretion can result in weight gain, peripheral edema, attenuation of the effects of antihypertensive agents, and rarely aggravation of congestive heart failure. Although rare, NSAIDs can cause hyponatremia by reducing renal free water clearance. Hyperkalemia could occur to a degree sufficient to cause cardiac arrhythmias. Renal function can decline sufficiently enough to cause acute renal failure. NSAIDs associated electrolyte and acid-base disturbances are not uncommon in some clinical situations. Adverse renal effects of NSAIDs are generally associated with prostaglandin dependent states such as volume-contracted states, low cardiac output, or other conditions that tend to compromise renal perfusion. All NSAIDs seem to share these adverse effects. In view of many NSAIDs users' susceptibility to renal adverse effects due to their underlying disease or condition, physicians should be cautious in prescribing NSAIDs to susceptible patients.
Keywords: Acute renal failure; Edema; Hyponatremia; Non-steroidal anti-inflammatory agents; Renal tubular acidosis.
Figures

References
-
- Oates JA, FitzGerald GA, Branch RA, Jackson EK, Knapp HR, Roberts LJ., 2nd Clinical implications of prostaglandin and thromboxane A2 formation (2) N Engl J Med. 1988;319:761–767. - PubMed
-
- Oates JA, FitzGerald GA, Branch RA, Jackson EK, Knapp HR, Roberts LJ., 2nd Clinical implications of prostaglandin and thromboxane A2 formation (1) N Engl J Med. 1988;319:689–698. - PubMed
-
- Whelton A. Renal aspects of treatment with con ventional nonsteroidal anti-inflammatory drugs versus cyclooxygenase-2-specific inhibitors. Am J Med. 2001;110(Suppl 3A):33S–42S. - PubMed
-
- Currie MG, Needleman P. Renal arachidonic acid metabolism. Annu Rev Physiol. 1984;46:327–341. - PubMed
Publication types
LinkOut - more resources
Full Text Sources