

Esophageal perforation following cervical spine surgery: A review with considerations in airway management
- PMID: 24459627
- PMCID: PMC3891196
- DOI: 10.4103/2229-5151.124164
Esophageal perforation following cervical spine surgery: A review with considerations in airway management
Abstract
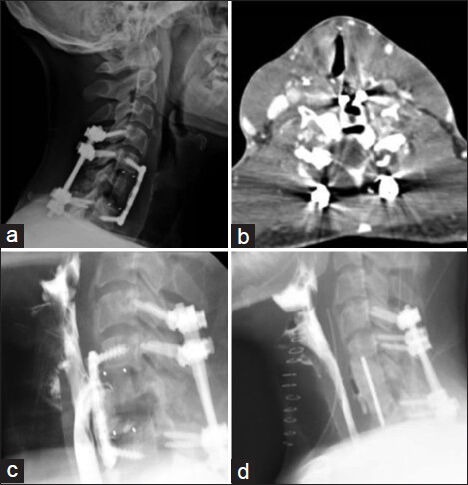
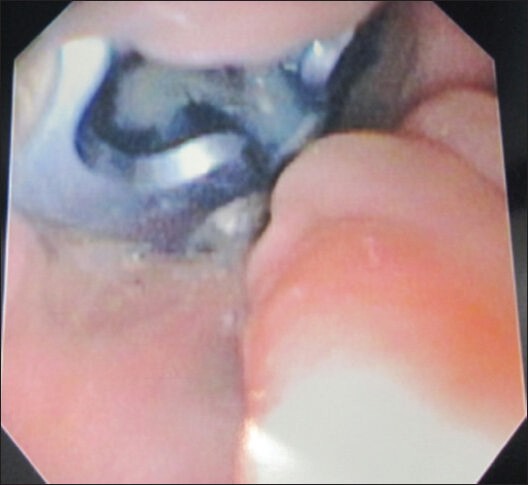
Anterior cervical discectomy and fusion (ACDF) is a commonly performed surgery for the treatment of spondylosis, radiculopathy, myelopathy, and trauma to the cervical spine. Esophageal perforation is a rare yet serious complication following ACDF with an incidence of 0.02 to 1.52%. We describe a case of a 24-year-old man who underwent ACDF and corpectomy following a motor vehicle accident who subsequently developed delayed onset esophageal perforation requiring surgical intervention. We believe that the detailed review of the surgical management of esophageal perforation following cervical spine surgery will provide a deeper understanding for the Intensivist in regards to postoperative airway management in these types of patients. Careful extubation over a soft flexible exchange catheter should take place to help reduce the risk of perforation in the event reintubation is required.
Keywords: Airway management; anterior cervical discectomy and Fusion; corpectomy; esophageal perforation.
Conflict of interest statement
Figures
References
-
- Ahn SH, Lee SH, Kim ES, Eoh W. Successful repair of esophageal perforation after anterior cervical fusion for cervical spine fracture. J Clin Neurosci. 2011;18:1374–80. - PubMed
-
- Dakwar E, Uribe JS, Padhya TA, Vale FL. Management of delayed esophageal perforations after anterior cervical spinal surgery. J Neurosurg Spine. 2009;11:320–5. - PubMed
-
- Haku T, Okuda S, Kanematsu F, Oda T, Miyauchi A, Yamamoto T, et al. Repair of cervical esophageal perforation using longus colli muscle flap: A case report of a patient with cervical spinal cord injury. Spine J. 2008;8:831–5. - PubMed
-
- Navarro R, Javahery R, Eismont F, Arnold DJ, Bhatia NN, Vanni S, et al. The role of the sternocleidomastoid muscle flap for esophageal fistula repair in anterior cervical spine surgery. Spine (Phila Pa 1976) 2005;30:E617–22. - PubMed
-
- Phommachanh V, Patil YJ, McCaffrey TV, Vale F, Freeman TB, Padhya TA. Otolaryngologic management of delayed pharyngoesophageal perforation following anterior cervical spine surgery. Laryngoscope. 2010;120:930–6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
