

Spousal diabetes as a diabetes risk factor: a systematic review and meta-analysis
- PMID: 24460622
- PMCID: PMC3900990
- DOI: 10.1186/1741-7015-12-12
Spousal diabetes as a diabetes risk factor: a systematic review and meta-analysis
Abstract
Background: Diabetes history in biologically-related individuals increases diabetes risk. We assessed diabetes concordance in spouses (that is, biologically unrelated family members) to gauge the importance of socioenvironmental factors.
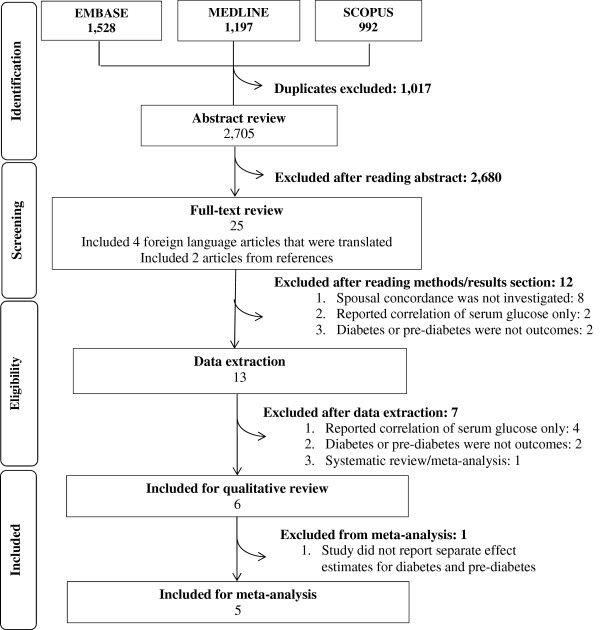
Methods: We selected cross-sectional, case-control and cohort studies examining spousal association for diabetes and/or prediabetes (impaired fasting glucose or impaired glucose tolerance), indexed in Medline, Embase or Scopus (1 January 1997 to 28 February 2013). Effect estimates (that is, odds ratios, incidence rate ratios, and so on) with body mass index (BMI) adjustment were pooled separately from those without BMI adjustment (random effects models) to distinguish BMI-dependent and independent concordance.
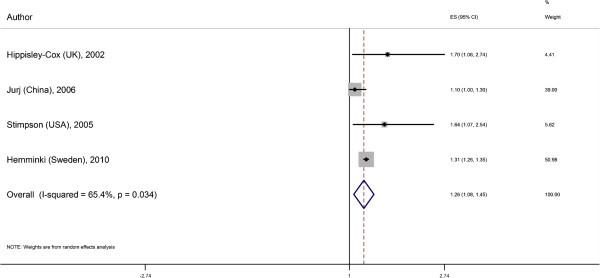
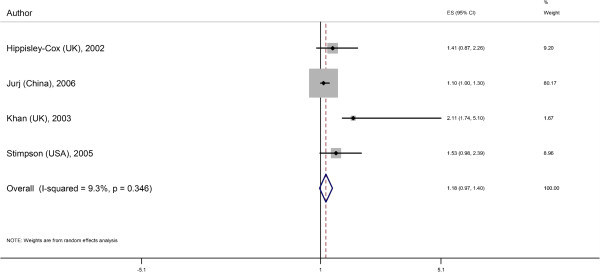
Results: Searches yielded 2,705 articles; six were retained (n = 75,498 couples) for systematic review and five for meta-analysis. Concordance was lowest in a study that relied on women's reports of diabetes in themselves and their spouses (effect estimate 1.1, 95% CI 1.0 to 1.30) and highest in a study with systematic assessment of glucose tolerance (2.11, 95% CI 1.74 to 5.10). The random-effects pooled estimate adjusted for age and other covariates but not BMI was 1.26 (95% CI 1.08 to 1.45). The estimate with BMI adjustment was lower (1.18, 95% CI 0.97 to 1.40). Two studies assessing between-spouse associations of diabetes/prediabetes determined by glucose testing reported high concordance (OR 1.92, 95% CI 1.55 to 2.37 without BMI adjustment; 2.32, 95% CI 1.87 to 3.98 with BMI adjustment). Two studies did not distinguish type 1 and type 2 diabetes. However given that around 95% of adults is type 2, this is unlikely to have influenced the results.
Conclusions: Our pooled estimate suggests that a spousal history of diabetes is associated with a 26% diabetes risk increase. Recognizing shared risk between spouses may improve diabetes detection and motivate couples to increase collaborative efforts to optimize eating and physical activity habits.
Figures
Comment in
-
Diabetes risk increased between spouses.Evid Based Nurs. 2015 Jan;18(1):28. doi: 10.1136/eb-2014-101784. Epub 2014 May 7. Evid Based Nurs. 2015. PMID: 24809938 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
