

Giant cell encephalitis and microglial infection with mucosally transmitted simian-human immunodeficiency virus SHIVSF162P3N in rhesus macaques
- PMID: 24464410
- PMCID: PMC4337388
- DOI: 10.1007/s13365-013-0229-z
Giant cell encephalitis and microglial infection with mucosally transmitted simian-human immunodeficiency virus SHIVSF162P3N in rhesus macaques
Abstract
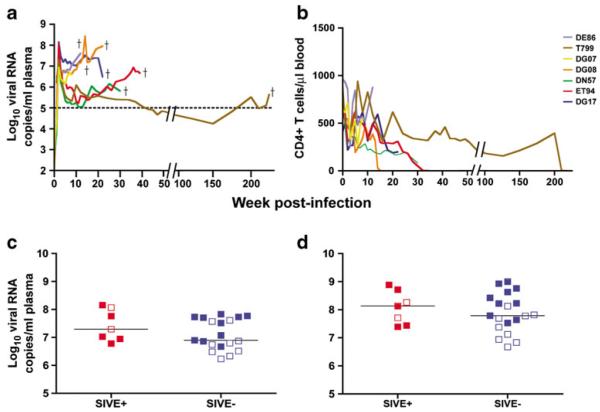
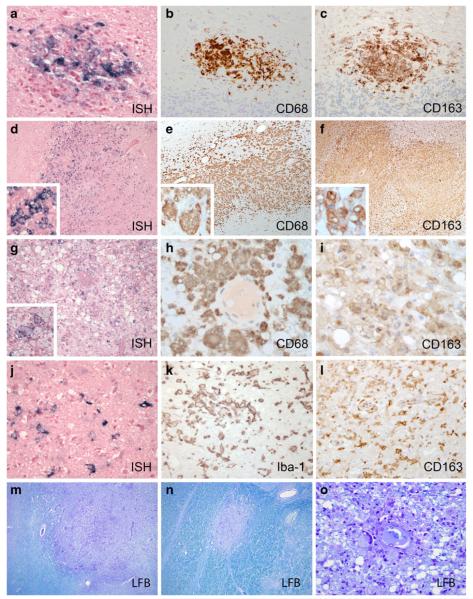
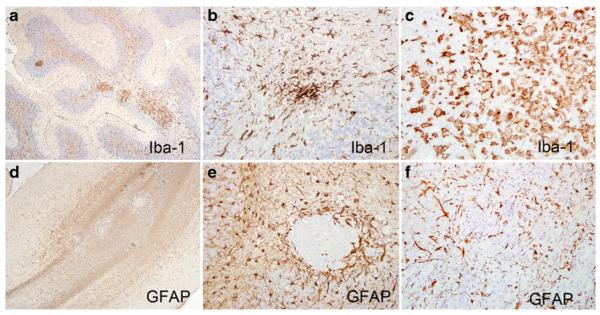
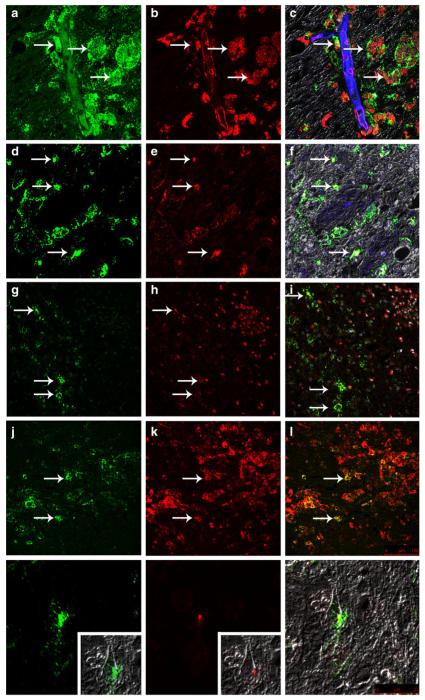
Neurocognitive disorders such as dementia and cognitive/motor impairments are among the most significant complications associated with human immunodeficiency virus (HIV) infection, especially in aging populations, yet the pathogenesis remains poorly understood. Activated macrophages and microglia in white matter along with the hallmark multinucleated giant cells are prominent features of HIV encephalitis (HIVE) and of several simian immunodeficiency virus (SIV) models. While infected microglia have been demonstrated in HIVE, this feature is not routinely seen in experimental infections in rhesus macaques using SIV or chimeric simian/HIV (SHIV) strains, limiting utility in HIV-1 pathogenesis and treatment studies. Here, 50 rhesus macaques were inoculated with the CCR5 (R5)-tropic SHIVSF162P3N virus by one of three routes: intravenously (n = 9), intrarectally (n = 17), or intravaginally (n = 24). Forty-three monkeys became viremic, 26 developed AIDS, and 7 (7/26, 27 %) developed giant cell SIV encephalitis (SIVE). Rapid progressor phenotype was evident in five of seven (71 %) macaques with SIVE, and expansion to utilize the CXCR4 coreceptor (X4 coreceptor switch) was observed in four out of seven (57 %). SIVE lesions were present in gray and white matter in the cerebrum, cerebellum, thalamus, and brain stem of affected animals. Lesions were composed of virally infected CD68(+), CD163(+), and HLA-DR(+) macrophages accompanied by white matter damage, necrosis, and astroglial and microglial activation. Importantly, microglial infection was observed, which makes R5 SHIVSF162P3N infection of macaques an attractive animal model not only to study transmission and HIVE pathogenesis but also to conduct preclinical evaluation of therapeutic interventions aimed at eradicating HIV-1 from the central nervous system (CNS).
Figures
References
-
- Annamalai L, Bhaskar V, Pauley DR, Knight H, Williams K, Lentz M, Ratai E, Westmoreland SV, Gonzalez RG, O’Neil SP. Impact of short-term combined antiretroviral therapy on brain virus burden in simian immunodeficiency virus-infected and CD8+ lymphocyte-depleted rhesus macaques. Am J Pathol. 2010;177:777–791. - PMC - PubMed
-
- Aquaro S, Calio R, Balzarini J, Bellocchi MC, Garaci E, Perno CF. Macrophages and HIV infection: therapeutical approaches toward this strategic virus reservoir. Antivir Res. 2002;55:209–225. - PubMed
-
- Budka H, Costanzi G, Cristina S, Lechi A, Parravicini C, Trabattoni R, Vago L. Brain pathology induced by infection with the human immunodeficiency virus (HIV). A histological, immunocytochemical, and electron microscopical study of 100 autopsy cases. Acta Neuropathol. 1987;75:185–198. - PubMed
-
- Churchill MJ, Wesselingh SL, Cowley D, Pardo CA, McArthur JC, Brew BJ, Gorry PR. Extensive astrocyte infection is prominent in human immunodeficiency virus-associated dementia. Ann Neurol. 2009;66:253–258. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
