

Implantable device diagnostics on day of discharge identify heart failure patients at increased risk for early readmission for heart failure
- PMID: 24464745
- PMCID: PMC4238830
- DOI: 10.1002/ejhf.48
Implantable device diagnostics on day of discharge identify heart failure patients at increased risk for early readmission for heart failure
Abstract
Aims: We hypothesized that diagnostic data in implantable devices evaluated on the day of discharge from a heart failure hospitalization (HFH) can identify patients at risk for HF readmission (HFR) within 30 days.
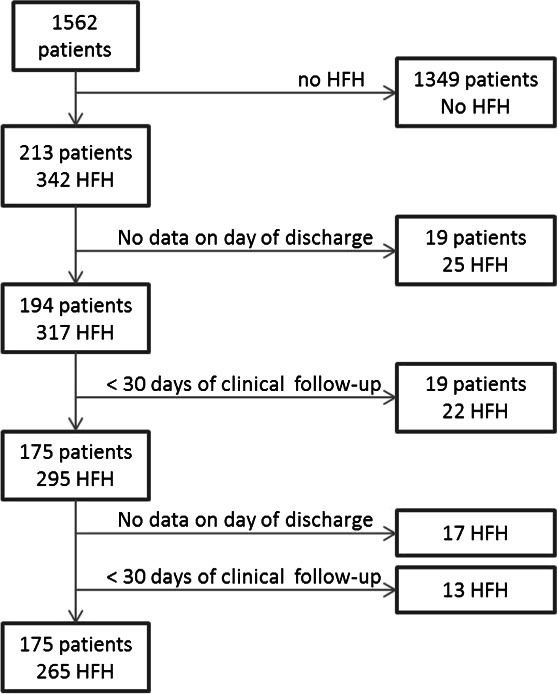
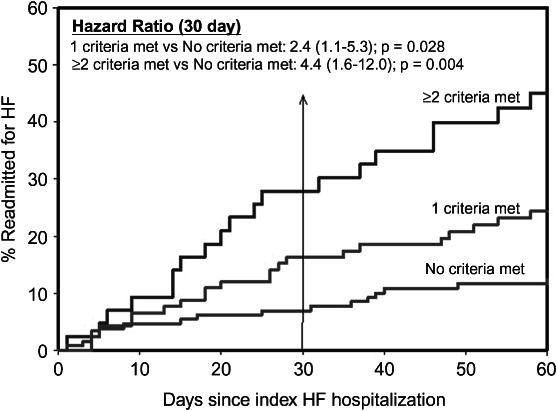
Methods and results: In this retrospective analysis of four studies enrolling patients with CRT devices, we identified patients with a HFH, device data on the day of discharge, and 30-day post-discharge clinical follow-up. Four diagnostic criteria were evaluated on the discharge day: (i) intrathoracic impedance>8 Ω below reference impedance; (ii) AF burden>6 h; (iii) CRT pacing<90%; and (iv) night heart rate>80 b.p.m. Patients were considered to have higher risk for HFR if ≥2 criteria were met, average risk if 1 criterion was met, and lower risk if no criteria were met. A Cox proportional hazards model was used to compare the groups. The data cohort consisted of a total of 265 HFHs in 175 patients, of which 36 (14%) were followed by HFR. On the discharge day, ≥2 criteria were met in 43 (16% of 265 HFHs), only 1 criterion was met in 92 (35%), and none of the four criteria were met in 130 HFHs (49%); HFR rates were 28, 16, and 7%, respectively. HFH with ≥2 criteria met was five times more likely to have HFR compared with HFH with no criteria met (adjusted hazard ratio 5.0; 95% confidence interval 1.9–13.5, P=0.001).
Conclusion: Device-derived diagnostic criteria evaluated on the day of discharge identified patients at significantly higher risk of HFR.
© 2013 The Authors. European Journal of Heart Failure
Figures
References
-
- McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez-Sanchez MA, Jaarsma T, Kober L, Lip GY, Maggioni AP, Parkhomenko A, Pieske BM, Popescu BA, Ronnevik PK, Rutten FH, Schwitter J, Seferovic P, Stepinska J, Trindade PT, Voors AA, Zannad F, Zeiher A, Bax JJ, Baumgartner H, Ceconi C, Dean V, Deaton C, Fagard R, Funck-Brentano C, Hasdai D, Hoes A, Kirchhof P, Knuuti J, Kolh P, McDonagh T, Moulin C, Reiner Z, Sechtem U, Sirnes PA, Tendera M, Torbicki A, Vahanian A, Windecker S, Bonet LA, Avraamides P, Ben Lamin HA, Brignole M, Coca A, Cowburn P, Dargie H, Elliott P, Flachskampf FA, Guida GF, Hardman S, Iung B, Merkely B, Mueller C, Nanas JN, Nielsen OW, Orn S, Parissis JT, Ponikowski P. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2012;14:803–869. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428. - PubMed
-
- McDonagh TA, Blue L, Clark AL, Dahlstrom U, Ekman I, Lainscak M, McDonald K, Ryder M, Stromberg A, Jaarsma T. European Society of Cardiology Heart Failure Association Standards for delivering heart failure care. Eur J Heart Fail. 2011;13:235–241. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
