

Anti-LGI1 Limbic Encephalitis Presented with Atypical Manifestations
- PMID: 24465150
- PMCID: PMC3897696
- DOI: 10.5607/en.2013.22.4.337
Anti-LGI1 Limbic Encephalitis Presented with Atypical Manifestations
Abstract
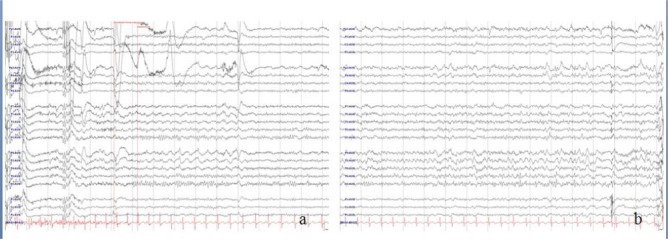
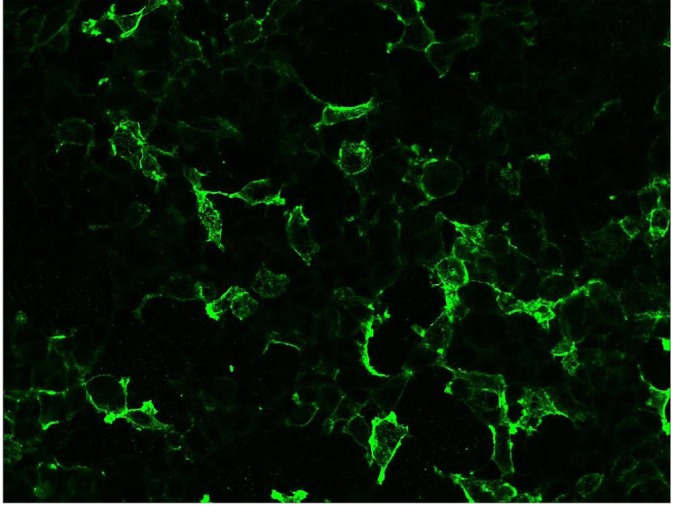
Anti-leucine-rich glioma inactivated-1 (LGI1) limbic encephalitis (LE) is a rare neurological disorder that has a subacute course of progressive encephalopathy and fasciobrachial dystonic seizures. We report a patient with anti-LGI1 LE that presented with atypical manifestations that complicated the diagnosis. A 62-year-old woman presented with a chronic course of memory disturbance and a subsequent relapse with an altered mental status after 10 months. The patient reported frequent chest pain of squeezing and dull nature, typically lasting 10-30 seconds. The chest pain was related to partial seizures, which were confirmed by video-EEG monitoring. Anti-LGI1 antibody was identified in serum and CSF. The patient's symptoms improved by immune modulation treatment. Patients with anti-LGI1 LE can experience atypical partial seizures, and a chronic relapsing course. Clinical suspicions and video-EEG monitoring are helpful for the early diagnosis and effective immune modulation.
Keywords: chest pain; immune; limbic encephalitis; seizure.
Figures
Similar articles
-
Acute Bilateral Vocal Cord Paralysis in a Patient With Anti-Leucine-Rich Glioma-Inactivated 1 (LGI1) Limbic Encephalitis.Cureus. 2024 Dec 10;16(12):e75475. doi: 10.7759/cureus.75475. eCollection 2024 Dec. Cureus. 2024. PMID: 39664290 Free PMC article.
-
A Case of Anti-Leucine-Rich Glioma-Inactivated Protein 1 (Anti-LGI1) Limbic Encephalitis With New-Onset Panic Attacks.Cureus. 2024 Apr 16;16(4):e58406. doi: 10.7759/cureus.58406. eCollection 2024 Apr. Cureus. 2024. PMID: 38756253 Free PMC article.
-
A Case of Anti-Leucine-Rich Glioma-Inactivated Protein 1 (Anti-LGI1) Limbic Encephalitis With Normal Imaging.Cureus. 2024 Jun 14;16(6):e62387. doi: 10.7759/cureus.62387. eCollection 2024 Jun. Cureus. 2024. PMID: 39006729 Free PMC article.
-
Three cases of antibody-LGI1 limbic encephalitis and review of literature.Int J Neurosci. 2019 Jul;129(7):642-648. doi: 10.1080/00207454.2018.1512985. Epub 2019 Mar 1. Int J Neurosci. 2019. PMID: 30112956 Review.
-
Clinical Features and Therapeutic Effects of Anti-leucine-rich Glioma Inactivated 1 Encephalitis: A Systematic Review.Front Neurol. 2022 Jan 12;12:791014. doi: 10.3389/fneur.2021.791014. eCollection 2021. Front Neurol. 2022. PMID: 35095736 Free PMC article.
Cited by
-
PIP-EL: A New Ensemble Learning Method for Improved Proinflammatory Peptide Predictions.Front Immunol. 2018 Jul 31;9:1783. doi: 10.3389/fimmu.2018.01783. eCollection 2018. Front Immunol. 2018. PMID: 30108593 Free PMC article.
-
Anti-Leucine-Rich Glioma-Inactivated 1 (Anti-LGI 1) Limbic Encephalitis and New-Onset Psychosis: A Case Report.Cureus. 2023 Mar 16;15(3):e36223. doi: 10.7759/cureus.36223. eCollection 2023 Mar. Cureus. 2023. PMID: 37069884 Free PMC article.
-
Possible anti-VGKC autoimmune limbic encephalitis associated with SIADH.BMJ Case Rep. 2018 Mar 7;2018:bcr2017223484. doi: 10.1136/bcr-2017-223484. BMJ Case Rep. 2018. PMID: 29514833 Free PMC article.
-
Case Report: Paroxysmal hyperhidrosis as an initial symptom in a patient with anti-LGI1 encephalitis.Front Immunol. 2022 Sep 23;13:986853. doi: 10.3389/fimmu.2022.986853. eCollection 2022. Front Immunol. 2022. PMID: 36211373 Free PMC article.
-
Anti-leucine-rich glioma-inactivated 1 limbic encephalitis: A case report and literature review.Exp Ther Med. 2016 Jan;11(1):315-317. doi: 10.3892/etm.2015.2866. Epub 2015 Nov 13. Exp Ther Med. 2016. PMID: 26889260 Free PMC article.
References
-
- Corsellis JA, Goldberg GJ, Norton AR. "Limbic encephalitis" and its association with carcinoma. Brain. 1968;91:481–496. - PubMed
-
- Graus F, Saiz A. Limbic encephalitis: a probably under-recognized syndrome. Neurologia. 2005;20:24–30. - PubMed
-
- Bien CG, Schulze-Bonhage A, Deckert M, Urbach H, Helmstaedter C, Grunwald T, Schaller C, Elger CE. Limbic encephalitis not associated with neoplasm as a cause of temporal lobe epilepsy. Neurology. 2000;55:1823–1828. - PubMed
-
- Tüzün E, Dalmau J. Limbic encephalitis and variants: classification, diagnosis and treatment. Neurologist. 2007;13:261–271. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
