

A risk prediction model for the assessment and triage of women with hypertensive disorders of pregnancy in low-resourced settings: the miniPIERS (Pre-eclampsia Integrated Estimate of RiSk) multi-country prospective cohort study
- PMID: 24465185
- PMCID: PMC3897359
- DOI: 10.1371/journal.pmed.1001589
A risk prediction model for the assessment and triage of women with hypertensive disorders of pregnancy in low-resourced settings: the miniPIERS (Pre-eclampsia Integrated Estimate of RiSk) multi-country prospective cohort study
Abstract
Background: Pre-eclampsia/eclampsia are leading causes of maternal mortality and morbidity, particularly in low- and middle- income countries (LMICs). We developed the miniPIERS risk prediction model to provide a simple, evidence-based tool to identify pregnant women in LMICs at increased risk of death or major hypertensive-related complications.
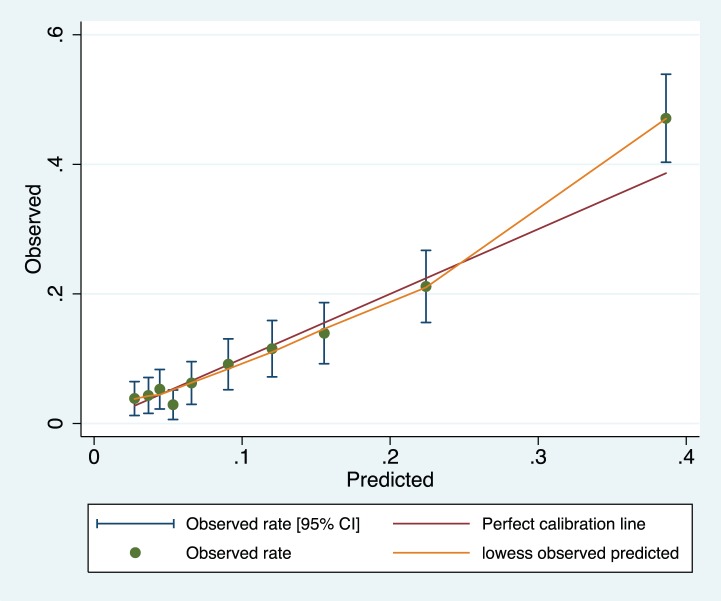
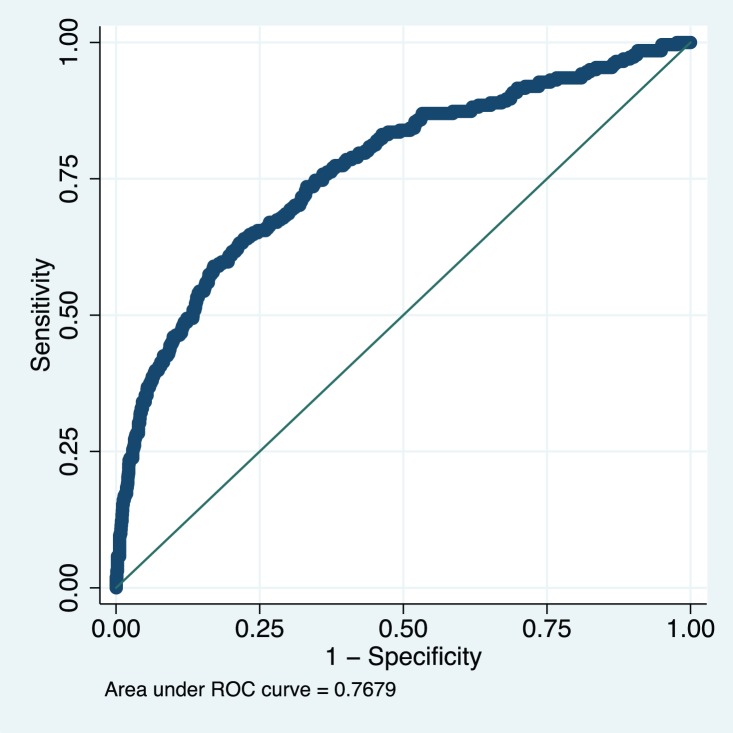
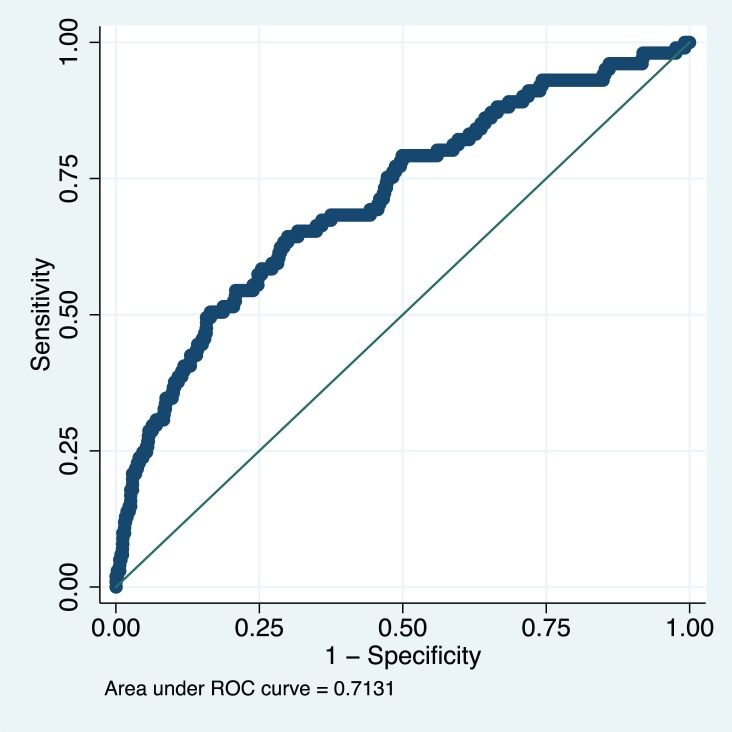
Methods and findings: From 1 July 2008 to 31 March 2012, in five LMICs, data were collected prospectively on 2,081 women with any hypertensive disorder of pregnancy admitted to a participating centre. Candidate predictors collected within 24 hours of admission were entered into a step-wise backward elimination logistic regression model to predict a composite adverse maternal outcome within 48 hours of admission. Model internal validation was accomplished by bootstrapping and external validation was completed using data from 1,300 women in the Pre-eclampsia Integrated Estimate of RiSk (fullPIERS) dataset. Predictive performance was assessed for calibration, discrimination, and stratification capacity. The final miniPIERS model included: parity (nulliparous versus multiparous); gestational age on admission; headache/visual disturbances; chest pain/dyspnoea; vaginal bleeding with abdominal pain; systolic blood pressure; and dipstick proteinuria. The miniPIERS model was well-calibrated and had an area under the receiver operating characteristic curve (AUC ROC) of 0.768 (95% CI 0.735-0.801) with an average optimism of 0.037. External validation AUC ROC was 0.713 (95% CI 0.658-0.768). A predicted probability ≥25% to define a positive test classified women with 85.5% accuracy. Limitations of this study include the composite outcome and the broad inclusion criteria of any hypertensive disorder of pregnancy. This broad approach was used to optimize model generalizability.
Conclusions: The miniPIERS model shows reasonable ability to identify women at increased risk of adverse maternal outcomes associated with the hypertensive disorders of pregnancy. It could be used in LMICs to identify women who would benefit most from interventions such as magnesium sulphate, antihypertensives, or transportation to a higher level of care.
Conflict of interest statement
PVD is a paid consultant of Alere International for work not related to the current manuscript; JMA is a founder of a startup company (LGTMedical) that is attempting to commercialize the development of a cell phone-based pulse oximeter; JMA holds <5% equity stake in the company. ZAB is a member of the Editorial Board of
Figures
References
-
- Steegers EA, von Dadelszen P, Duvekot JJ, Pijnenborg R (2010) Pre-eclampsia. Lancet 376: 631–644. - PubMed
-
- Khan KS, Wojdyla D, Say L, Gulmezoglu AM, Van Look PF (2006) WHO analysis of causes of maternal death: a systematic review. Lancet 367: 1066–1074. - PubMed
-
- Hutcheon JA, Lisonkova S, Joseph KS (2011) Epidemiology of pre-eclampsia and the other hypertensive disorders of pregnancy. Best Pract Res Clin Obstet Gynaecol 25: 391–403. - PubMed
-
- Firoz T, Sanghvi H, Merialdi M, von Dadelszen P (2011) Pre-eclampsia in low and middle income countries. Best Pract Res Clin Obstet Gynaecol 25: 537–548. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
