

Toll-like receptor 4 stimulation before or after Streptococcus pneumoniae induced sepsis improves survival and is dependent on T-cells
- PMID: 24465843
- PMCID: PMC3897608
- DOI: 10.1371/journal.pone.0086015
Toll-like receptor 4 stimulation before or after Streptococcus pneumoniae induced sepsis improves survival and is dependent on T-cells
Abstract
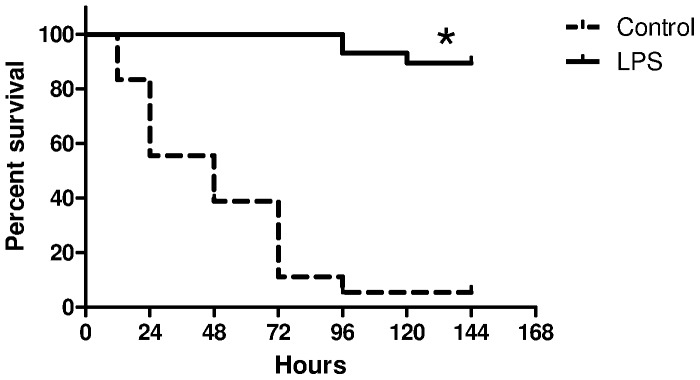
Introduction: Endotoxin tolerance improves outcomes from gram negative sepsis but the underlying mechanism is not known. We determined if endotoxin tolerance before or after pneumococcal sepsis improved survival and the role of lymphocytes in this protection.
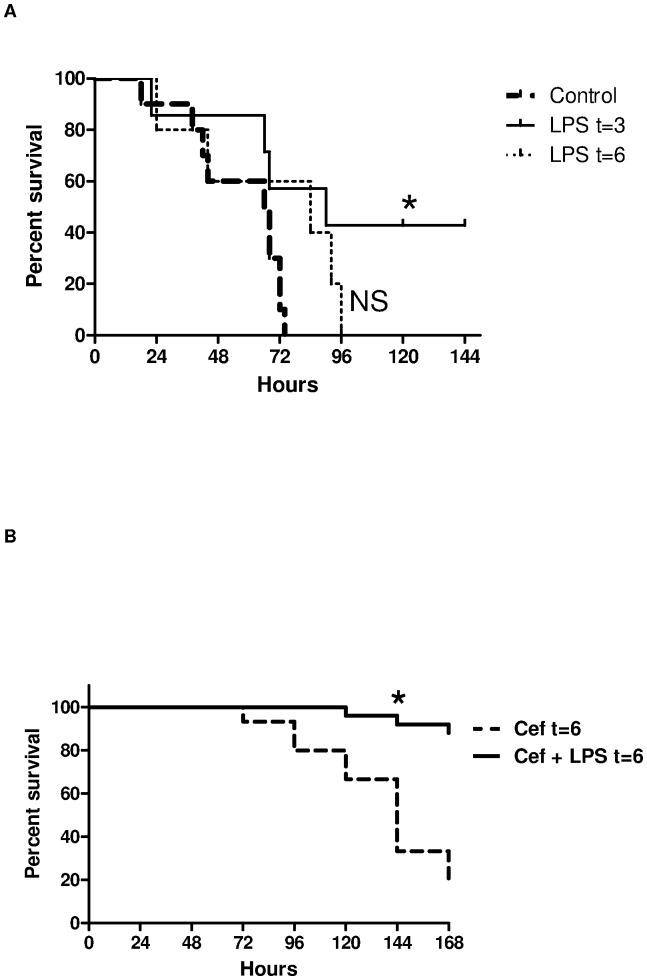
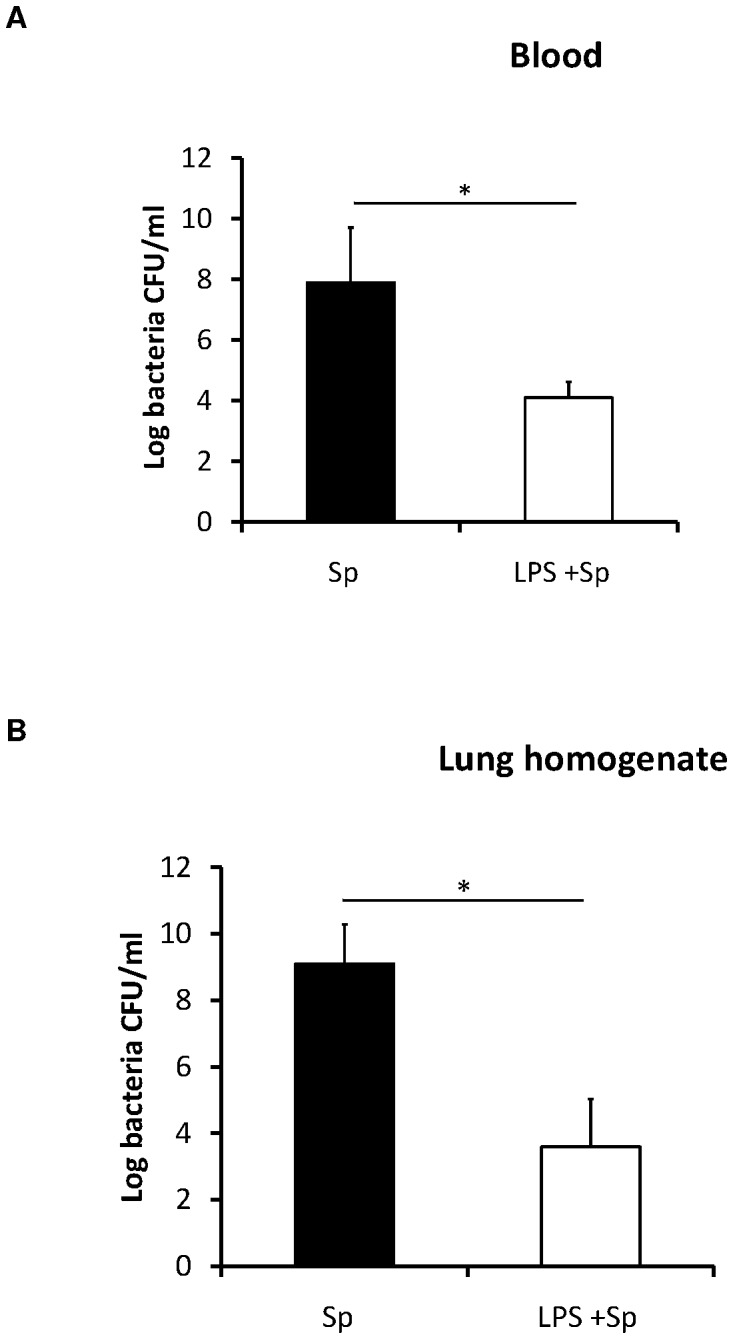
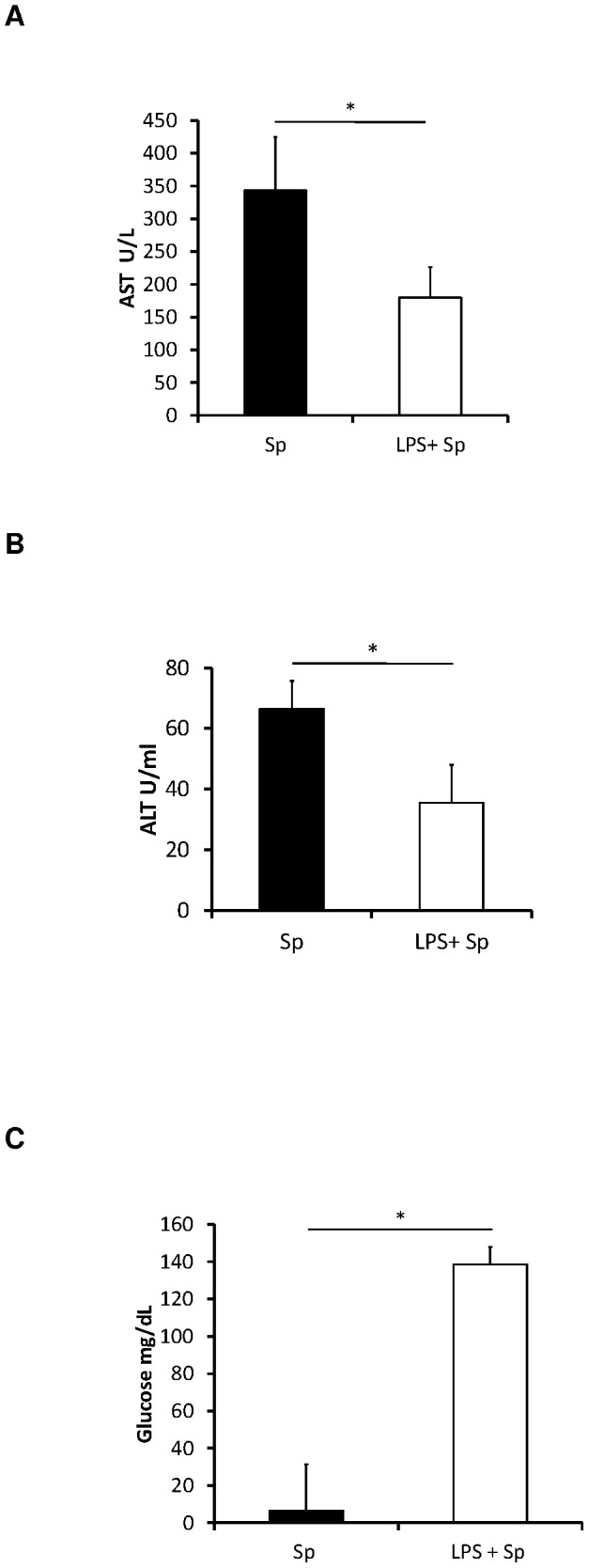
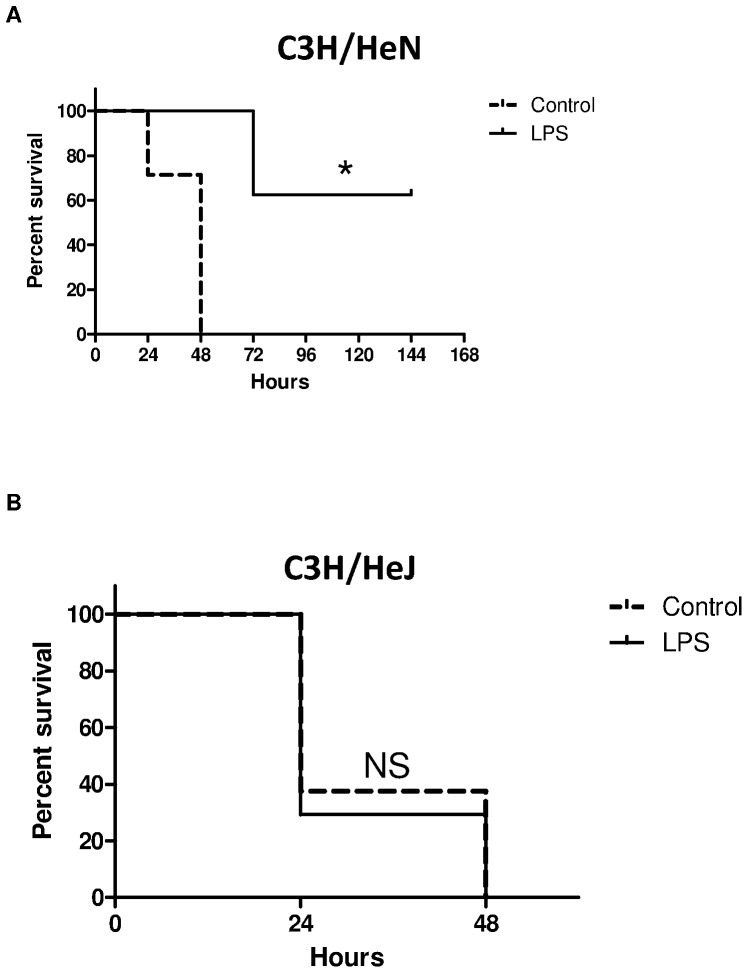
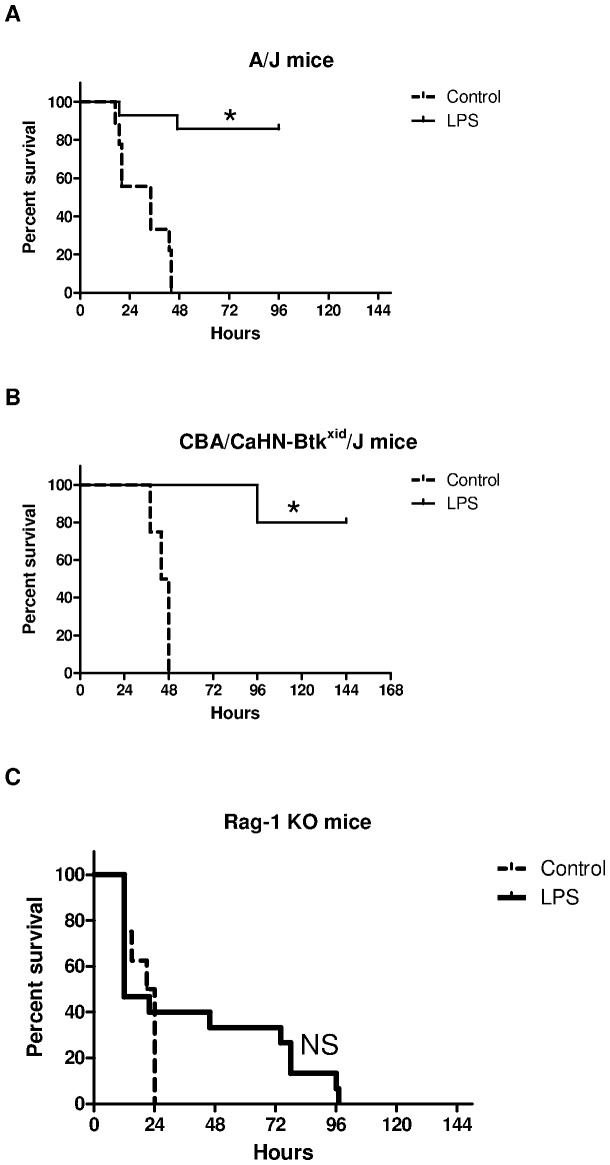
Methods: Mice received lipopolysaccharide (LPS) or vehicle before or after a lethal dose of Streptococcus pneumoniae. Survival, quantitative bacteriology, liver function, and cytokine concentrations were measured. We confirmed the necessity of Toll-like receptor 4 (TLR4) for endotoxin tolerance using C3H/HeN (TLR4 replete) and C3H/HeJ (TLR4 deficient) mice. The role of complement was investigated through A/J mice deficient in C5 complement. CBA/CaHN-Btk(xid/)/J mice with dysfunctional B cells and Rag-1 knockout (KO) mice deficient in T and B cells delineated the role of lymphocytes.
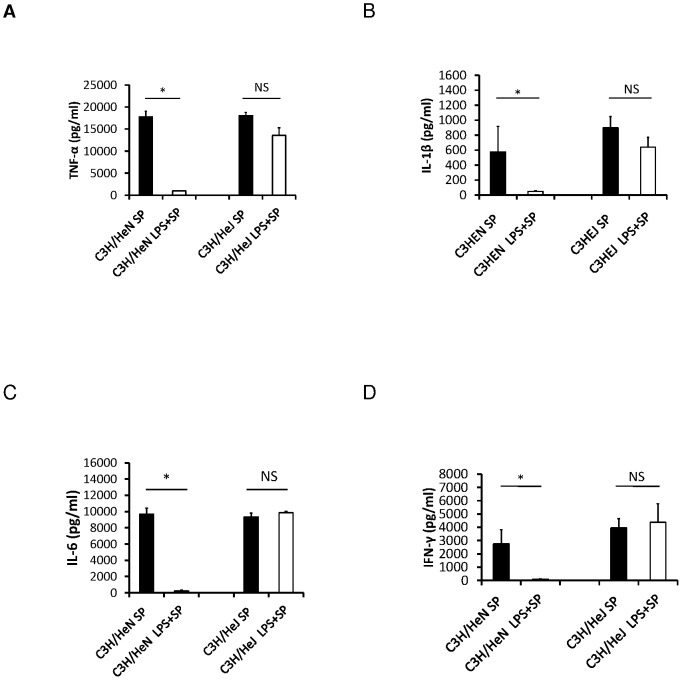
Results: Endotoxin tolerance improved survival from pneumococcal sepsis in mice with TLR4 that received LPS pretreatment or posttreatment. Survival was associated with reduced bacterial burden and serum cytokine concentrations. Death was associated with abnormal liver function and blood glucose concentrations. Endotoxin tolerance improved survival in A/J and CBA/CaHN-Btk(xid/)/J mice but not Rag-1 KO mice.
Conclusions: TLR4 stimulation before or after S. pneumoniae infection improved survival and was dependent on T-cells but did not require an intact complement cascade or functional B cells.
Conflict of interest statement
Figures
References
-
- Martin GS, Mannino DM, Eaton S, Moss M (2003) The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med 348: 1546–1554. - PubMed
-
- Appelbaum PC (2002) Resistance among Streptococcus pneumoniae: Implications for drug selection. Clin Infect Dis 34: 1613–1620. - PubMed
-
- Dremsizov T, Clermont G, Kellum JA, Kalassian KG, Fine MJ, et al. (2006) Severe sepsis in community-acquired pneumonia: when does it happen, and do systemic inflammatory response syndrome criteria help predict course? Chest 129: 968–978. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
