

Age-dependent prevalence of nasopharyngeal carriage of streptococcus pneumoniae before conjugate vaccine introduction: a prediction model based on a meta-analysis
- PMID: 24465920
- PMCID: PMC3900487
- DOI: 10.1371/journal.pone.0086136
Age-dependent prevalence of nasopharyngeal carriage of streptococcus pneumoniae before conjugate vaccine introduction: a prediction model based on a meta-analysis
Abstract
Introduction: Data on the prevalence of nasopharyngeal carriage of S.pneumoniae in all age groups are important to help predict the impact of introducing pneumococcal conjugate vaccines (PCV) into routine infant immunization, given the important indirect effect of the vaccine. Yet most carriage studies are limited to children under five years of age. We here explore the association between carriage prevalence and serotype distribution in children aged ≥5 years and in adults compared to children.
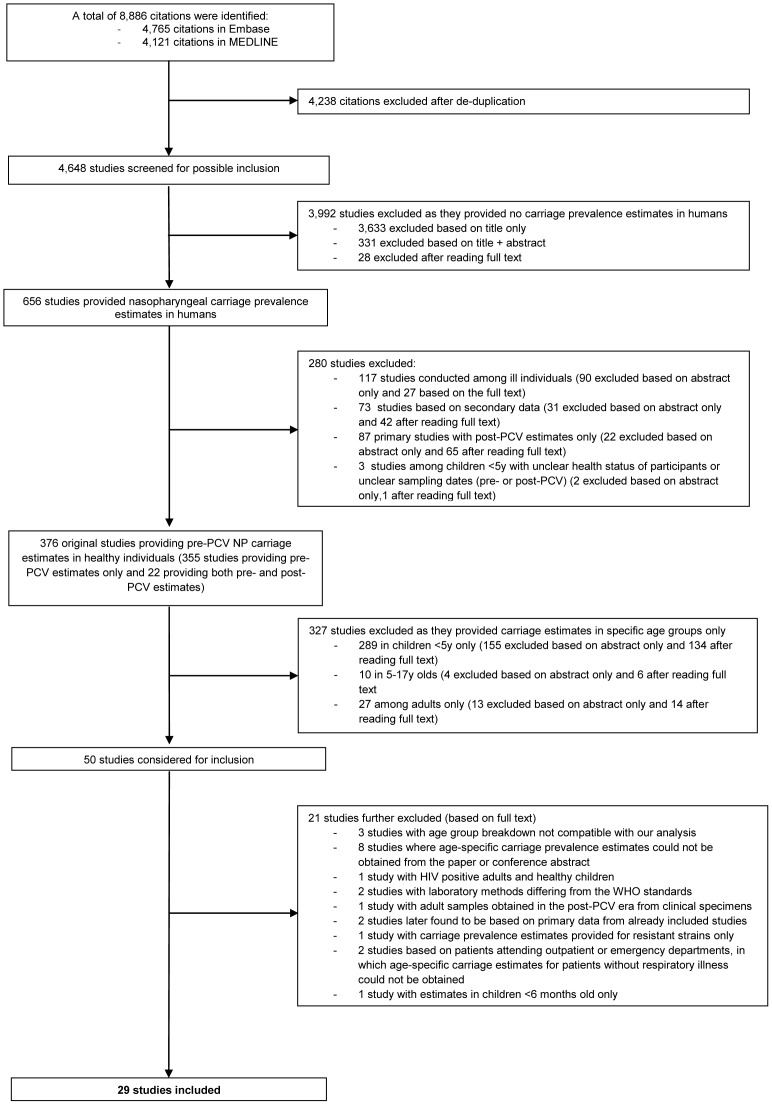
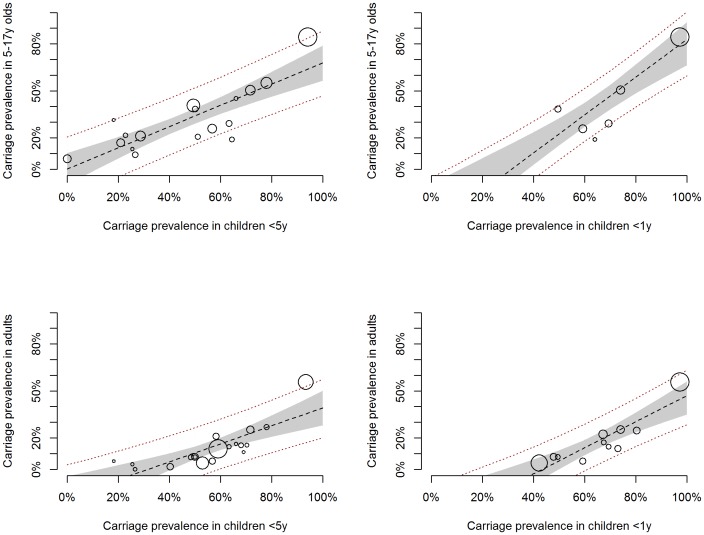
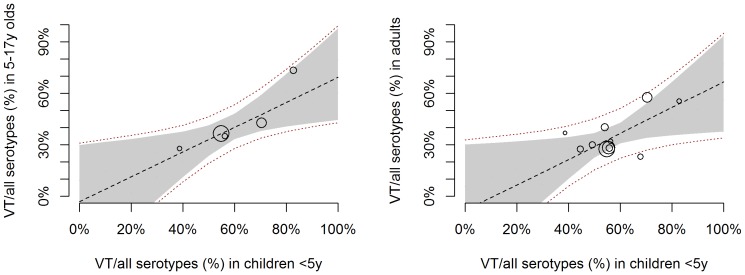
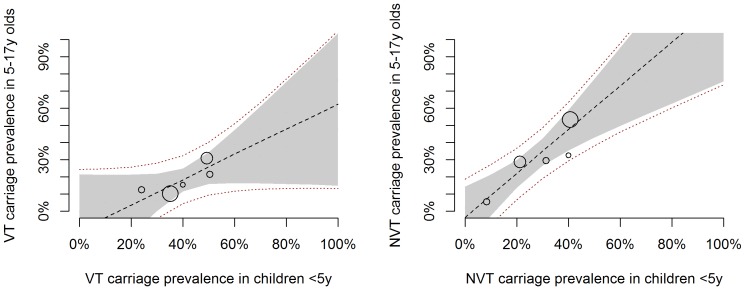
Methods: We conducted a systematic review of studies providing carriage estimates across age groups in healthy populations not previously exposed to PCV, using MEDLINE and Embase. We used Bayesian linear meta-regression models to predict the overall carriage prevalence as well as the prevalence and distribution of vaccine and nonvaccine type (VT and NVT) serotypes in older age groups as a function of that in <5 y olds.
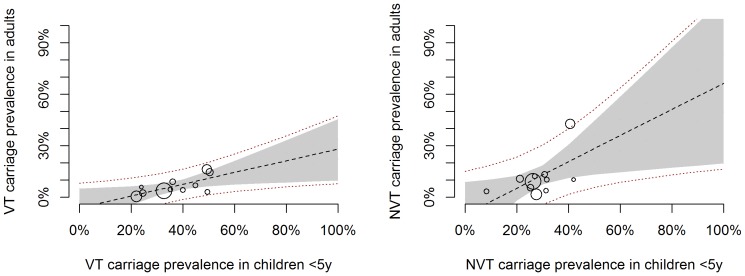
Results: Twenty-nine studies compromising of 20,391 individuals were included in the analysis. In all studies nasopharyngeal carriage decreased with increasing age. We found a strong positive linear association between the carriage prevalence in pre-school childen (<5 y) and both that in school aged children (5-17 y olds) and in adults. The proportion of VT serotypes isolated from carriers was consistently lower in older age groups and on average about 73% that of children <5 y among 5-17 y olds and adults respectively. We provide a prediction model to infer the carriage prevalence and serotype distribution in 5-17 y olds and adults as a function of that in children <5 years of age.
Conclusion: Such predictions are helpful for assessing the potential population-wide effects of vaccination programmes, e.g. via transmission models, and thus assist in the design of future pneumococcal conjugate vaccination strategies.
Conflict of interest statement
Figures
References
-
- Bogaert D, De Groot R, Hermans PW (2004) Streptococcus pneumoniae colonisation: the key to pneumococcal disease. Lancet Infect Dis 4: 144–154. - PubMed
-
- Halasa NB, Grijalva CG, Arbogast PG, Talbot TR, Craig AS, et al... (2013) Near Complete Elimination of the Seven Valent Pneumococcal Conjugate Vaccine Serotypes in Tennessee. Pediatr Infect Dis J. - PubMed
-
- Hammitt LL, Bruden DL, Butler JC, Baggett HC, Hurlburt DA, et al. (2006) Indirect effect of conjugate vaccine on adult carriage of Streptococcus pneumoniae: an explanation of trends in invasive pneumococcal disease. JInfectDis 193: 1487–1494. - PubMed
-
- Fitzwater SP, Chandran A, Santosham M, Johnson HL (2012) The worldwide impact of the seven-valent pneumococcal conjugate vaccine. Pediatr Infect Dis J 31: 501–508. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
