

A multidisciplinary intervention to reduce infections of ESBL- and AmpC-producing, gram-negative bacteria at a University Hospital
- PMID: 24466106
- PMCID: PMC3900527
- DOI: 10.1371/journal.pone.0086457
A multidisciplinary intervention to reduce infections of ESBL- and AmpC-producing, gram-negative bacteria at a University Hospital
Abstract
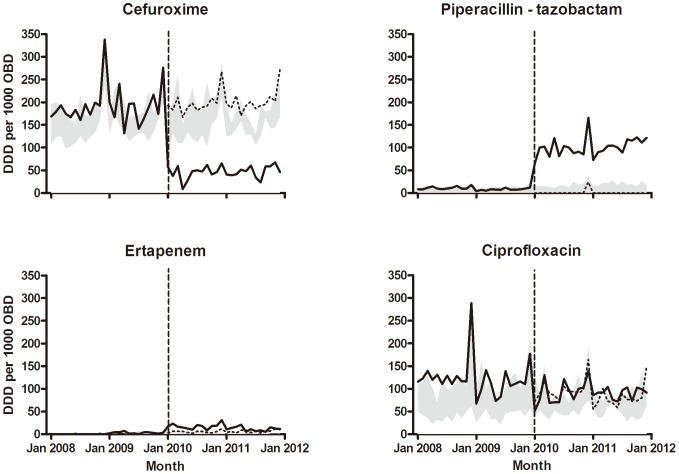
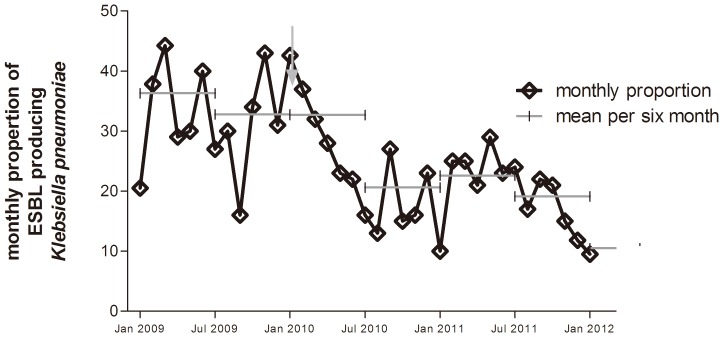
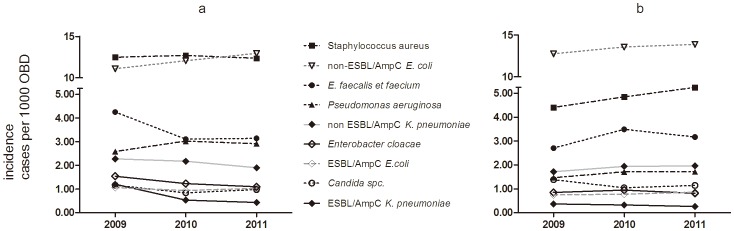
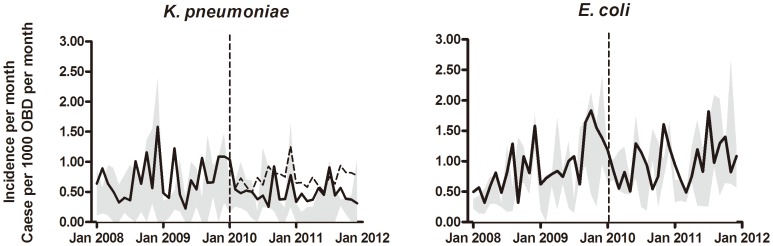
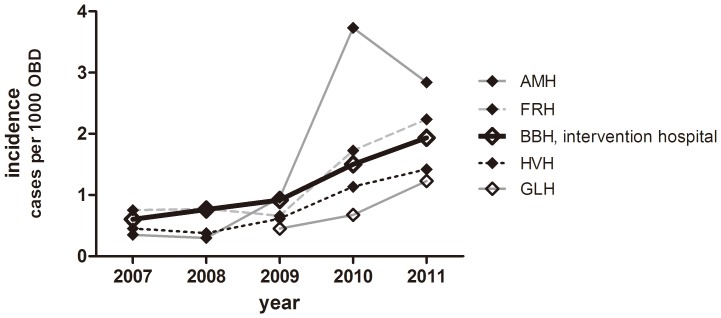
In response to a considerable increase in the infections caused by ESBL/AmpC-producing Klebsiella pneumonia in 2008, a multidisciplinary intervention, with a main focus on antimicrobial stewardship, was carried out at one university hospital. Four other hospitals were used as controls. Stringent guidelines for antimicrobial treatment and prophylaxis were disseminated throughout the intervention hospital; cephalosporins were restricted for prophylaxis use only, fluoroquinolones for empiric use in septic shock only, and carbapenems were selected for penicillin-allergic patients, infections due to ESBL/AmpC-producing and other resistant bacteria, in addition to their use in severe sepsis/septic shock. Piperacillin-tazobactam ± gentamicin was recommended for empiric treatments of most febrile conditions. The intervention also included education and guidance on infection control, as well as various other surveillances. Two year follow-up data on the incidence rates of patients with selected bacterial infections, outcomes, and antibiotic consumption were assessed, employing before-and-after analysis and segmented regression analysis of interrupted time series, using the other hospitals as controls. The intervention led to a sustained change in antimicrobial consumption, and the incidence of patients infected with ESBL-producing K. pneumoniae decreased significantly (p<0.001). The incidences of other hospital-associated infections also declined (p's<0.02), but piperacillin-tazobactam-resistant Pseudomonas aeruginosa and Enterococcus faecium infections increased (p's<0.033). In wards with high antimicrobial consumption, the patient gut carrier rate of ESBL-producing bacteria significantly decreased (p = 0.023). The unadjusted, all-cause 30-day mortality rates of K. pneumoniae and E. coli were unchanged over the four-year period, with similar results in all five hospitals. Although not statistically significant, the 30-day mortality rate of patients with ESBL-producing K. pneumoniae decreased, from 35% in 2008-2009, to 17% in 2010-2011. The two-year follow-up data indicated that this multidisciplinary intervention led to a statistically significant decrease in the incidence of ESBL/AmpC-resistant K. pneumoniae infections, as well as in the incidences of other typical hospital-associated bacterial infections.
Conflict of interest statement
Figures
References
-
- European Centre for Disease Prevention and Control (2011) Antimicrobial resistance surveillance in Europe 2010. Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net). Stockholm: ECDC.
-
- Gupta N, Patel JB, Kallen AJ (2011) Carbapenem-resistant Enterobacteriaceae: epidemiology and prevention.Clin. Infect Dis 53: 60–67. - PubMed
-
- Pitout JDD (2010) Infections with extended-spectrum beta-lactamase-producing enterobacteriaceae: changing epidemiology and drug treatment choises. Drugs 70: 313–33. - PubMed
-
- Schwaber MJ, Carmeli Y (2007) Mortality and delay in effective therapy associated with extended-spectrum beta-lactamase production in Enterobateriaceae bacteraemia: a systematic review and metaanlysis. J Antimicrob Chemother 60: 913–920. - PubMed
-
- Panhotra BR, Saxena A, Al-Ghamdi AM (2004) Extended-spectrum beta-lactamase producing Klebsiella pneumoniae hospital acquired bacteremia. Risk factors and clinical outcome. Saudi Med J 25: 1871–1876. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
