

Noninvasive prenatal testing: the future is now
- PMID: 24466384
- PMCID: PMC3893900
Noninvasive prenatal testing: the future is now
Abstract
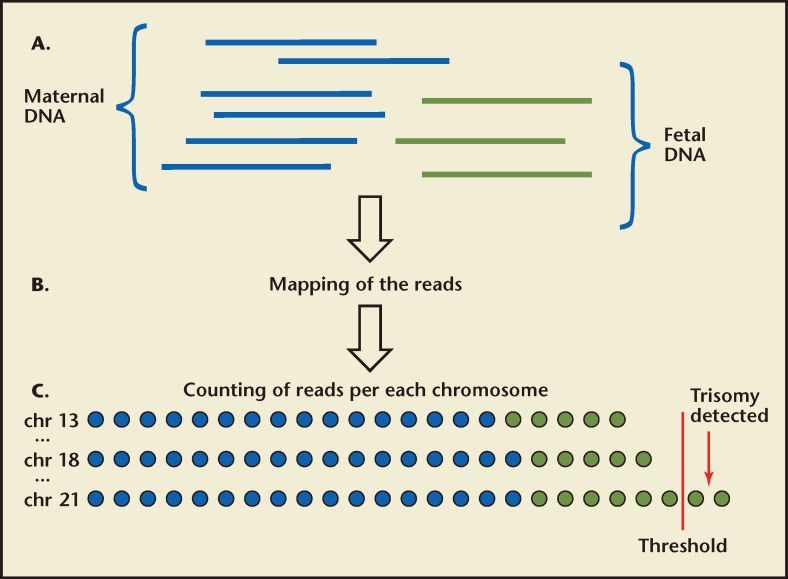
Prenatal detection of chromosome abnormalities has been offered for more than 40 years, first by amniocentesis in the early 1970s and additionally by chorionic villus sampling (CVS) in the early 1980s. Given the well-recognized association between increasing maternal age and trisomy,1-3 the primary utilization of prenatal testing has been by older mothers. This has drastically reduced the incidence of aneuploid children born to older mothers.4 Although younger women have relatively low risks of conceiving a child with aneuploidy, the majority of pregnant women are in their late teens, 20s, and early 30s. As such, most viable aneuploid babies are born to these younger mothers.5 Invasive prenatal diagnosis (CVS and amniocentesis) is not a feasible option for all low-risk mothers, as these procedures carry a small but finite risk and would ultimately cause more miscarriages than they would detect aneuploidy. For this reason, a number of noninvasive tests have been developed-including first-trimester risk assessment at 11 to 14 weeks, maternal serum analyte (quad) screening at 15 to 20 weeks, and sonographic fetal structural survey at 18 to 22 weeks-all of which are designed to give a woman an adjusted (more accurate) estimate of having an aneuploid fetus using as baseline her a priori age-related risk. Ultrasound and maternal serum analysis are considered screening procedures and both require follow up by CVS or amniocentesis in screen-positive cases for a definitive diagnosis of a chromosome abnormality in the fetus. The ability to isolate fetal cells and fetal DNA from maternal blood during pregnancy has opened up exciting opportunities for improved noninvasive prenatal testing (NIPT). Direct analysis of fetal cells from maternal circulation has been challenging given the scarcity of fetal cells in maternal blood (1:10,000-1:1,000,000) and the focus has shifted to the analysis of cell-free fetal DNA, which is found at a concentration almost 25 times higher than that available from nucleated blood cells extracted from a similar volume of whole maternal blood. There have now been numerous reports on the use of cell-free DNA (cfDNA) for NIPT for chromosomal aneuploidies-especially trisomy (an extra copy of a chromosome) or monosomy (a missing chromosome)-and a number of commercial products are already being marketed for this indication. This article reviews the various techniques being used to analyze cell-free DNA in the maternal circulation for the prenatal detection of chromosome abnormalities and the evidence in support of each. A number of areas of ongoing controversy are addressed, including the timing of maternal blood sampling, the need for genetic counseling, and the use of confirmatory invasive testing. Future applications for this technology are also reviewed.
Keywords: Cell-free fetal DNA; Noninvasive prenatal testing; Prenatal diagnosis; Trisomy 21.
Figures
References
-
- Hassold T, Hunt PA, Sherman S. Trisomy in humans: incidence, origin and etiology. Curr Opin Genet Dev. 1993;3:398–403. - PubMed
-
- Penrose LS. The relative aetiological importance of birth order and maternal age in mongolism. Proc Roy Soc Lond [Biol] 1934;115:431–450.
-
- Sherman SL, Petersen MB, Freeman SB, et al. Nondisjunction of chromosome 21 in maternal meiosis I: evidence for a maternal age-dependent mechanism involving reduced recombination. Hum Mol Genet. 1994;3:1529–1535. - PubMed
-
- Hook EB. Chromosome abnormalities: prevalence, risks and recurrence. In: Brock DJH, Rodeck CH, Ferguson-Smith MA, editors. Prenatal Diagnosis and Screening. Edinburgh, Scotland: Churchill Livingstone; 1992. pp. 351–392.
-
- Gardner RJM, Sutherland GR. Chromosome Abnormalities and Genetic Counseling. New York, NY: Oxford University Press; 1996. p. 478.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources