

Threshold of Clinical Severity of Cervical Dystonia for Positive (18)F-FDG PET/CT
- PMID: 24466512
- PMCID: PMC3895517
- DOI: 10.5535/arm.2013.37.6.777
Threshold of Clinical Severity of Cervical Dystonia for Positive (18)F-FDG PET/CT
Abstract
Objective: To examine whether the clinical severity of cervical dystonia (CD) significantly correlates with (18)F-fluorodeoxyglucose positron emission tomography/computed tomography ((18)F-FDG PET/CT) findings as well as to determine the threshold of the clinical severity of CD for positive (18)F-FDG PET/CT study findings.
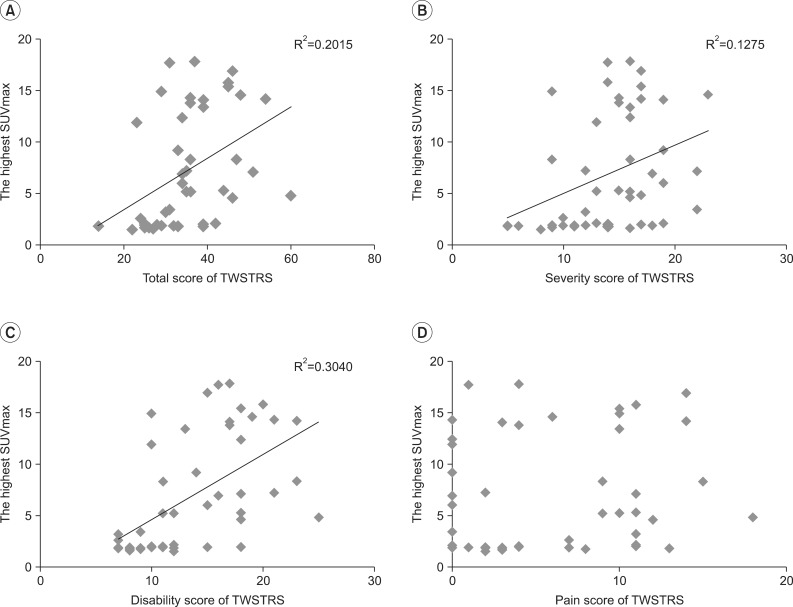
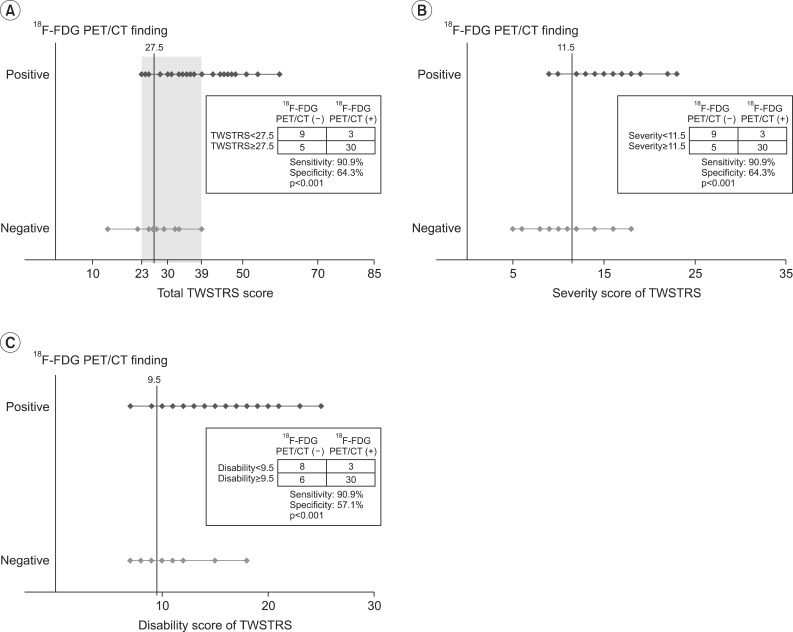
Methods: Forty-seven subjects with torticollis as one of the symptoms of CD were included. The clinical severity of CD was evaluated with the Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) at the time of (18)F-FDG PET/CT. The correlation between the clinical severity of CD and the highest SUVmax was examined. The threshold of the clinical severity of CD necessary for positive (18)F-FDG PET/CT findings was determined using receiver operating characteristics curve analysis.
Results: Thirty-three of the 47 subjects (70.21%) showed positive (18)F-FDG PET/CT findings. The ipsilateral splenius capitis/cervicis, oblique capitis inferior, and longus colli/capitis were the rotators most frequently involved. The highest SUVmax of (18)F-FDG PET/CT was significant correlated with the TWSTRS. Subjects with a total TWSTRS exceeding 39 showed positive (18)F-FDG PET/CT findings, with those having a total TWSTRS ≤22 showing negative (18)F-FDG PET/CT results. The cutoff value of the total TWSTRS for positive (18)F-FDG PET/CT findings was set at 27.5 with 90.9% sensitivity and 64.3% specificity.
Conclusion: A significant correlation was evident between the clinical severity of CD and (18)F-FDG PET/CT findings, providing a threshold of the clinical severity of CD for acquisition of positive (18)F-FDG PET/CT findings.
Keywords: Cervical dystonia; Fluorodeoxyglucose F18; Positron-emission tomography.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Usefulness of (18)f-fluorodeoxyglucose positron emission tomography/computed tomography in management of cervical dystonia.Ann Rehabil Med. 2012 Dec;36(6):745-55. doi: 10.5535/arm.2012.36.6.745. Epub 2012 Dec 28. Ann Rehabil Med. 2012. PMID: 23342305 Free PMC article.
-
Therapeutic Efficacy and Prediction of 18F-FDG PET/CT-Assisted Botulinum Toxin Therapy in Patients With Idiopathic Cervical Dystonia.Clin Nucl Med. 2022 Dec 1;47(12):e725-e730. doi: 10.1097/RLU.0000000000004383. Epub 2022 Sep 6. Clin Nucl Med. 2022. PMID: 36342802
-
Myotomy and Selective Peripheral Denervation Based on 18F-FDG PET/CT in Intractable Cervical Dystonia: A Case Report.NMC Case Rep J. 2023 Apr 10;10:99-102. doi: 10.2176/jns-nmc.2022-0392. eCollection 2023. NMC Case Rep J. 2023. PMID: 37131496 Free PMC article.
-
Diagnostic accuracy of F-18 FDG PET or PET/CT for detection of lymph node metastasis in clinically node negative head and neck cancer patients; A systematic review and meta-analysis.Am J Otolaryngol. 2019 Mar-Apr;40(2):297-305. doi: 10.1016/j.amjoto.2018.10.013. Epub 2018 Oct 23. Am J Otolaryngol. 2019. PMID: 30473166
-
A systematic review and meta-analysis of 18F-fluoro-d-deoxyglucose positron emission tomography interpretation methods in vascular graft and endograft infection.J Vasc Surg. 2020 Dec;72(6):2174-2185.e2. doi: 10.1016/j.jvs.2020.05.065. Epub 2020 Jul 6. J Vasc Surg. 2020. PMID: 32645420
Cited by
-
Muscle Function, Muscle Disease, and Positron Emission Tomography-Computed Tomography: A Narrative Review.Cureus. 2025 Feb 28;17(2):e79857. doi: 10.7759/cureus.79857. eCollection 2025 Feb. Cureus. 2025. PMID: 40166518 Free PMC article. Review.
-
A methodological approach for botulinum neurotoxin injections to the longus colli muscle in dystonic anterocollis: A case series of 4 patients and a literature review.J Clin Neurosci. 2020 Oct;80:188-194. doi: 10.1016/j.jocn.2020.08.025. Epub 2020 Aug 26. J Clin Neurosci. 2020. PMID: 33099344 Free PMC article. Review.
References
-
- Jankovic J, Tolosa E. Parkinson's disease and movement disorders. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2007.
-
- Jankovic J, Tsui J, Bergeron C. Prevalence of cervical dystonia and spasmodic torticollis in the United States general population. Parkinsonism Relat Disord. 2007;13:411–416. - PubMed
-
- Epidemiological Study of Dystonia in Europe (ESDE) Collaborative Group. A prevalence study of primary dystonia in eight European countries. J Neurol. 2000;247:787–792. - PubMed
-
- Camargo CH, Teive HA, Becker N, Baran MH, Scola RH, Werneck LC. Cervical dystonia: clinical and therapeutic features in 85 patients. Arq Neuropsiquiatr. 2008;66:15–21. - PubMed
-
- Albanese A, Barnes MP, Bhatia KP, Fernandez-Alvarez E, Filippini G, Gasser T, et al. A systematic review on the diagnosis and treatment of primary (idiopathic) dystonia and dystonia plus syndromes: report of an EFNS/MDS-ES Task Force. Eur J Neurol. 2006;13:433–444. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
