

Botulinum toxin in the treatment of drooling in tetraplegic patients with brain injury
- PMID: 24466514
- PMCID: PMC3895519
- DOI: 10.5535/arm.2013.37.6.796
Botulinum toxin in the treatment of drooling in tetraplegic patients with brain injury
Abstract
Objective: To investigate the effect of botulinum toxin type A (BTA) injection into the salivary gland and to evaluate the changes of drooling in varied postures in tetraplegic patients with brain injury.
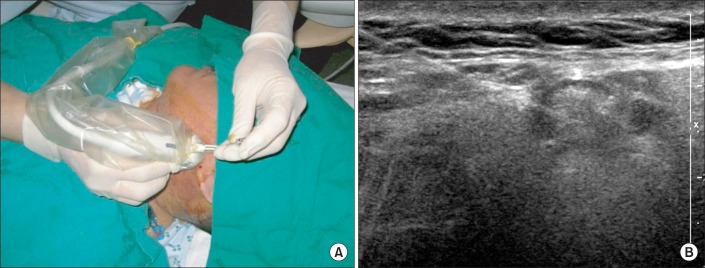
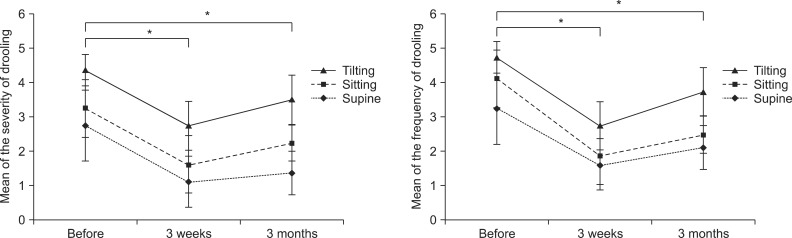
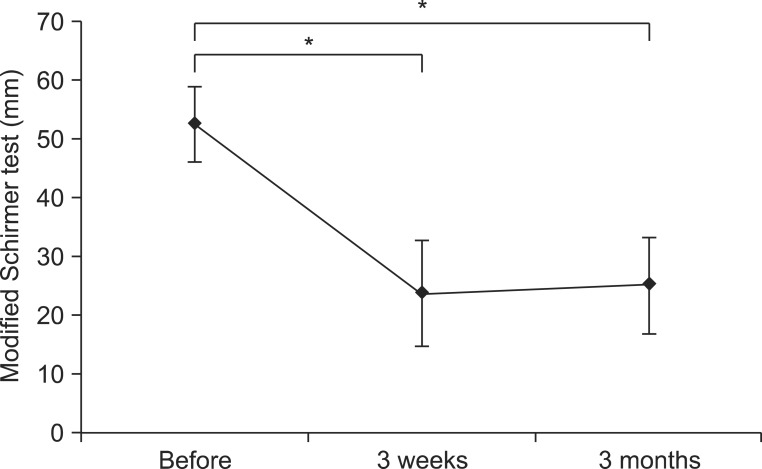
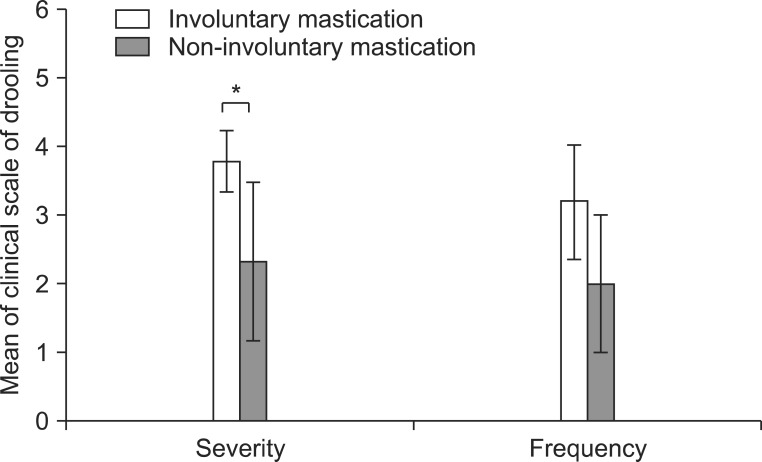
Methods: Eight tetraplegic patients with brain injury were enrolled. BTA was injected into each parotid and submandibular gland of both sides under ultrasonographic guidance. Drooling was measured by a questionnaire-based scoring system for drooling severity and frequency, and the sialorrhea was measured by a modified Schirmer test for the patients before the injection, 3 weeks and 3 months after the injection. Drooling was evaluated in each posture, such as supine, sitting, and tilt table standing, and during involuntary mastication, before and after the injection.
Results: The severity and frequency of drooling and the modified Schirmer test improved significantly at 3 weeks and 3 months after the injection (p<0.05). Drooling was more severe and frequent in tilt table standing than in the sitting position and in sitting versus supine position (p<0.05). The severity of drooling was significantly increased in the patients with involuntary mastication (p<0.05).
Conclusion: Salivary gland injection of BTA in patients with tetraplegia resulting from brain injury who had drooling and sialorrhea could improve the symptoms for 3 months without complications. The severity and frequency of drooling were dependent on posture and involuntary mastication. Proper posture and involuntary mastication of the patients should be taken into account in planning drooling treatment.
Keywords: Botulinum toxins; Drooling; Posture; Salivary glands; Ultrasonography.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures

References
-
- Lim M, Mace A, Nouraei SA, Sandhu G. Botulinum toxin in the management of sialorrhoea: a systematic review. Clin Otolaryngol. 2006;31:267–272. - PubMed
-
- Thomas-Stonell N, Greenberg J. Three treatment approaches and clinical factors in the reduction of drooling. Dysphagia. 1988;3:73–78. - PubMed
-
- van der Burg JJ, Jongerius PH, van Limbeek J, van Hulst K, Rotteveel JJ. Social interaction and self-esteem of children with cerebral palsy after treatment for severe drooling. Eur J Pediatr. 2006;165:37–41. - PubMed
-
- Suskind DL, Tilton A. Clinical study of botulinum-A toxin in the treatment of sialorrhea in children with cerebral palsy. Laryngoscope. 2002;112:73–81. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
