

Efficacy of face shields against cough aerosol droplets from a cough simulator
- PMID: 24467190
- PMCID: PMC4734356
- DOI: 10.1080/15459624.2013.877591
Efficacy of face shields against cough aerosol droplets from a cough simulator
Abstract
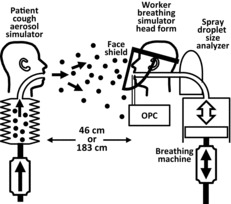
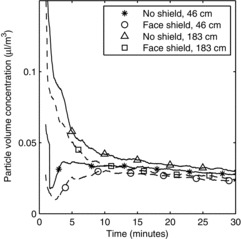
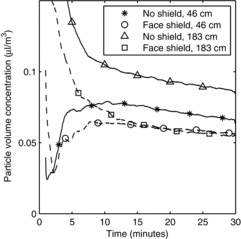
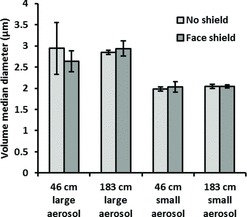
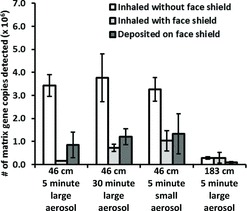
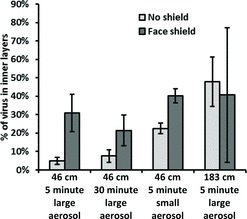
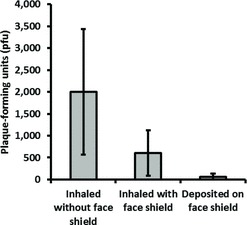
Health care workers are exposed to potentially infectious airborne particles while providing routine care to coughing patients. However, much is not understood about the behavior of these aerosols and the risks they pose. We used a coughing patient simulator and a breathing worker simulator to investigate the exposure of health care workers to cough aerosol droplets, and to examine the efficacy of face shields in reducing this exposure. Our results showed that 0.9% of the initial burst of aerosol from a cough can be inhaled by a worker 46 cm (18 inches) from the patient. During testing of an influenza-laden cough aerosol with a volume median diameter (VMD) of 8.5 μm, wearing a face shield reduced the inhalational exposure of the worker by 96% in the period immediately after a cough. The face shield also reduced the surface contamination of a respirator by 97%. When a smaller cough aerosol was used (VMD = 3.4 μm), the face shield was less effective, blocking only 68% of the cough and 76% of the surface contamination. In the period from 1 to 30 minutes after a cough, during which the aerosol had dispersed throughout the room and larger particles had settled, the face shield reduced aerosol inhalation by only 23%. Increasing the distance between the patient and worker to 183 cm (72 inches) reduced the exposure to influenza that occurred immediately after a cough by 92%. Our results show that health care workers can inhale infectious airborne particles while treating a coughing patient. Face shields can substantially reduce the short-term exposure of health care workers to large infectious aerosol particles, but smaller particles can remain airborne longer and flow around the face shield more easily to be inhaled. Thus, face shields provide a useful adjunct to respiratory protection for workers caring for patients with respiratory infections. However, they cannot be used as a substitute for respiratory protection when it is needed. [Supplementary materials are available for this article. Go to the publisher's online edition of Journal of Occupational and Environmental Hygiene for the following free supplemental resource: tables of the experiments performed, more detailed information about the aerosol measurement methods, photographs of the experimental setup, and summaries of the experimental data from the aerosol measurement devices, the qPCR analysis, and the VPA.].
Keywords: airborne particulate matter; health care workers; infectious disease transmission; protective devices; respiratory infections/prevention; universal precautions.
Figures


Comment in
-
A Customized Face-Shield for Ophthalmologists During COVID-19 Second Wave.Ophthalmic Plast Reconstr Surg. 2021 Jan-Feb 01;37(1):91-92. doi: 10.1097/IOP.0000000000001900. Ophthalmic Plast Reconstr Surg. 2021. PMID: 33395195 Free PMC article. No abstract available.
References
-
- McCool F.D.: Global physiology and pathophysiology of cough: ACCP evidence-based clinical practice guidelines. Chest 129(1 Suppl):48S–53S (2006). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical