

A loss of telocytes accompanies fibrosis of multiple organs in systemic sclerosis
- PMID: 24467430
- PMCID: PMC3930412
- DOI: 10.1111/jcmm.12228
A loss of telocytes accompanies fibrosis of multiple organs in systemic sclerosis
Abstract
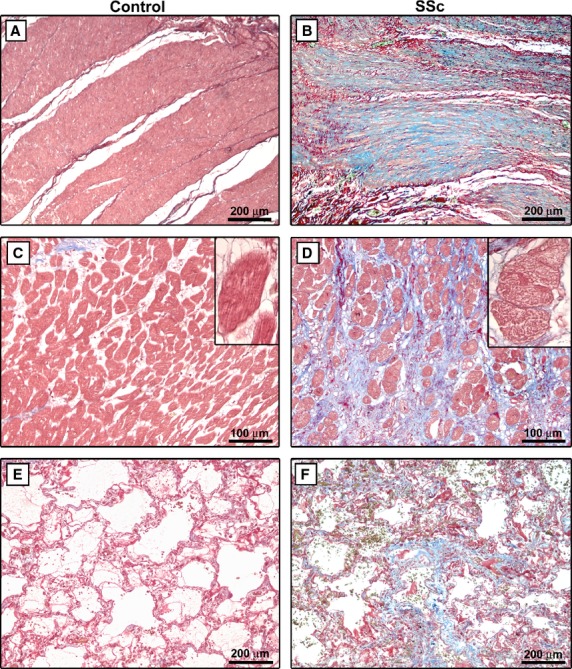
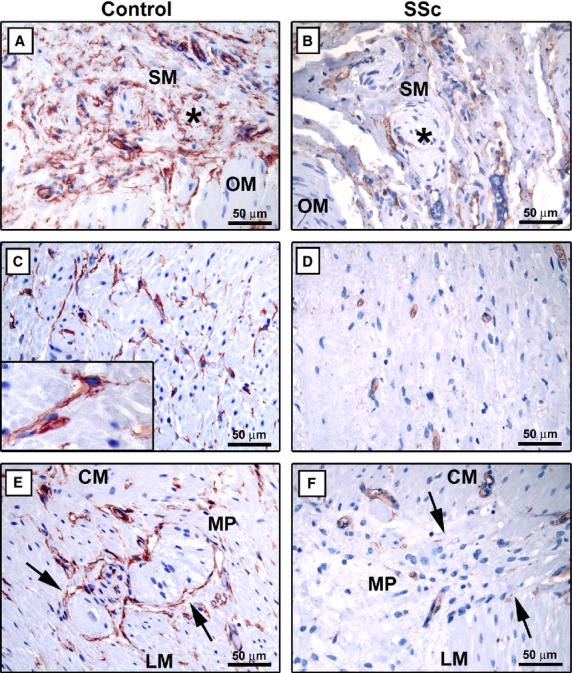
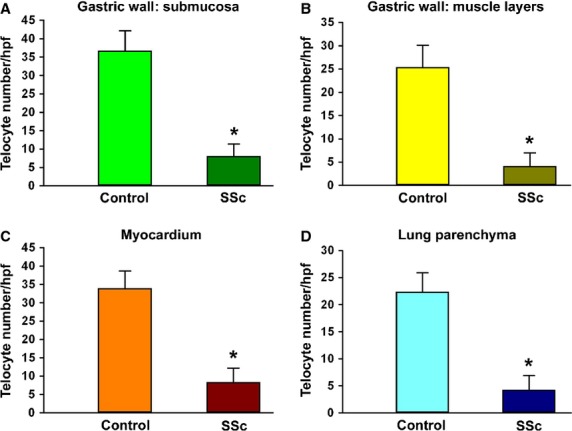
Systemic sclerosis (SSc) is a complex connective tissue disease characterized by fibrosis of the skin and various internal organs. In SSc, telocytes, a peculiar type of stromal (interstitial) cells, display severe ultrastructural damages and are progressively lost from the clinically affected skin. The aim of the present work was to investigate the presence and distribution of telocytes in the internal organs of SSc patients. Archival paraffin-embedded samples of gastric wall, myocardium and lung from SSc patients and controls were collected. Tissue sections were stained with Masson's trichrome to detect fibrosis. Telocytes were studied on tissue sections subjected to CD34 immunostaining. CD34/CD31 double immunofluorescence was performed to unequivocally differentiate telocytes (CD34-positive/CD31-negative) from vascular endothelial cells (CD34-positive/CD31-positive). Few telocytes entrapped in the fibrotic extracellular matrix were found in the muscularis mucosae and submucosa of SSc gastric wall. In the muscle layers and myenteric plexus, the network of telocytes was discontinuous or even completely absent around smooth muscle cells and ganglia. Telocytes were almost completely absent in fibrotic areas of SSc myocardium. In SSc fibrotic lung, few or no telocytes were observed in the thickened alveolar septa, around blood vessels and in the interstitial space surrounding terminal and respiratory bronchioles. In SSc, the loss of telocytes is not restricted to the skin, but it is a widespread process affecting multiple organs targeted by the fibrotic process. As telocytes are believed to be key players in the regulation of tissue/organ homoeostasis, our data suggest that telocyte loss might have important pathophysiological implications in SSc.
Keywords: CD34; fibrosis; gastric wall; immunohistochemistry; lung; myocardium; scleroderma; systemic sclerosis; telocytes.
© 2014 The Authors. Journal of Cellular and Molecular Medicine published by John Wiley & Sons Ltd and Foundation for Cellular and Molecular Medicine.
Figures



Similar articles
-
Evidence for progressive reduction and loss of telocytes in the dermal cellular network of systemic sclerosis.J Cell Mol Med. 2013 Apr;17(4):482-96. doi: 10.1111/jcmm.12028. Epub 2013 Feb 27. J Cell Mol Med. 2013. PMID: 23444845 Free PMC article.
-
Telocytes are reduced during fibrotic remodelling of the colonic wall in ulcerative colitis.J Cell Mol Med. 2015 Jan;19(1):62-73. doi: 10.1111/jcmm.12457. Epub 2014 Oct 6. J Cell Mol Med. 2015. PMID: 25283476 Free PMC article.
-
Scleroderma-like Impairment in the Network of Telocytes/CD34+ Stromal Cells in the Experimental Mouse Model of Bleomycin-Induced Dermal Fibrosis.Int J Mol Sci. 2021 Nov 17;22(22):12407. doi: 10.3390/ijms222212407. Int J Mol Sci. 2021. PMID: 34830288 Free PMC article.
-
Endothelial to mesenchymal transition (EndoMT) in the pathogenesis of Systemic Sclerosis-associated pulmonary fibrosis and pulmonary arterial hypertension. Myth or reality?Matrix Biol. 2016 Apr;51:26-36. doi: 10.1016/j.matbio.2016.01.012. Epub 2016 Jan 22. Matrix Biol. 2016. PMID: 26807760 Free PMC article. Review.
-
The Cutaneous Telocytes.Adv Exp Med Biol. 2016;913:303-323. doi: 10.1007/978-981-10-1061-3_20. Adv Exp Med Biol. 2016. PMID: 27796896 Review.
Cited by
-
Update on scleroderma-associated interstitial lung disease.Curr Opin Rheumatol. 2014 Nov;26(6):630-6. doi: 10.1097/BOR.0000000000000111. Curr Opin Rheumatol. 2014. PMID: 25191993 Free PMC article. Review.
-
Ultrastructural identification of telocytes in the muscularis of chicken ileum.Exp Ther Med. 2015 Dec;10(6):2325-2330. doi: 10.3892/etm.2015.2841. Epub 2015 Oct 30. Exp Ther Med. 2015. PMID: 26668636 Free PMC article.
-
Transcriptomic and histological characterization of telocytes in the human dorsal root ganglion.bioRxiv [Preprint]. 2024 Sep 24:2024.09.24.614693. doi: 10.1101/2024.09.24.614693. bioRxiv. 2024. Update in: J Comp Neurol. 2025 Mar;533(3):e70044. doi: 10.1002/cne.70044. PMID: 39386553 Free PMC article. Updated. Preprint.
-
Dynamic Involvement of Telocytes in Modulating Multiple Signaling Pathways in Cardiac Cytoarchitecture.Int J Mol Sci. 2022 May 21;23(10):5769. doi: 10.3390/ijms23105769. Int J Mol Sci. 2022. PMID: 35628576 Free PMC article. Review.
-
Telocytes: current methods of research, challenges and future perspectives.Cell Tissue Res. 2024 May;396(2):141-155. doi: 10.1007/s00441-024-03888-5. Epub 2024 Mar 28. Cell Tissue Res. 2024. PMID: 38539007 Review.
References
-
- Gabrielli A, Avvedimento EV, Krieg T. Scleroderma. N Engl J Med. 2009;360:1989–2003. - PubMed
-
- Jain S, Shahane A, Derk CT. Interstitial lung disease in systemic sclerosis: pathophysiology, current and new advances in therapy. Inflamm Allergy Drug Targets. 2012;11:266–77. - PubMed
-
- du Bois RM. Mechanisms of scleroderma-induced lung disease. Proc Am Thorac Soc. 2007;4:434–8. - PubMed
-
- Meune C, Vignaux O, Kahan A, et al. Heart involvement in systemic sclerosis: evolving concept and diagnostic methodologies. Arch Cardiovasc Dis. 2010;103:46–52. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
