

Stool substitute transplant therapy for the eradication of Clostridium difficile infection: 'RePOOPulating' the gut
- PMID: 24467987
- PMCID: PMC3869191
- DOI: 10.1186/2049-2618-1-3
Stool substitute transplant therapy for the eradication of Clostridium difficile infection: 'RePOOPulating' the gut
Abstract
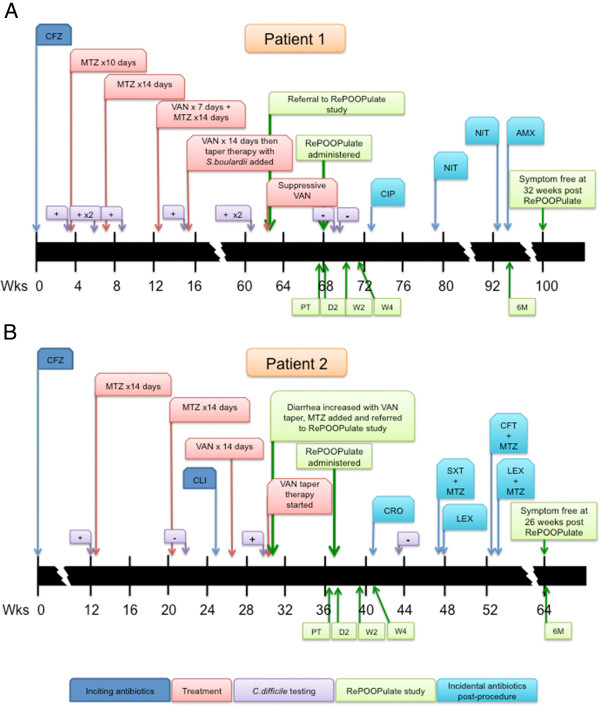
Background: Fecal bacteriotherapy ('stool transplant') can be effective in treating recurrent Clostridium difficile infection, but concerns of donor infection transmission and patient acceptance limit its use. Here we describe the use of a stool substitute preparation, made from purified intestinal bacterial cultures derived from a single healthy donor, to treat recurrent C. difficile infection that had failed repeated standard antibiotics. Thirty-three isolates were recovered from a healthy donor stool sample. Two patients who had failed at least three courses of metronidazole or vancomycin underwent colonoscopy and the mixture was infused throughout the right and mid colon. Pre-treatment and post-treatment stool samples were analyzed by 16 S rRNA gene sequencing using the Ion Torrent platform.
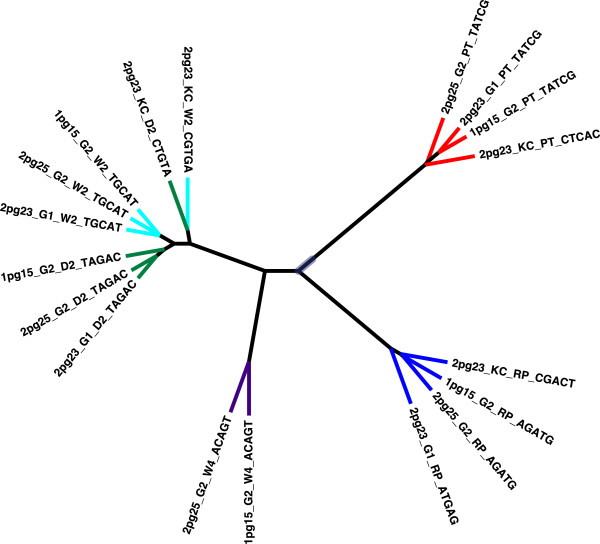
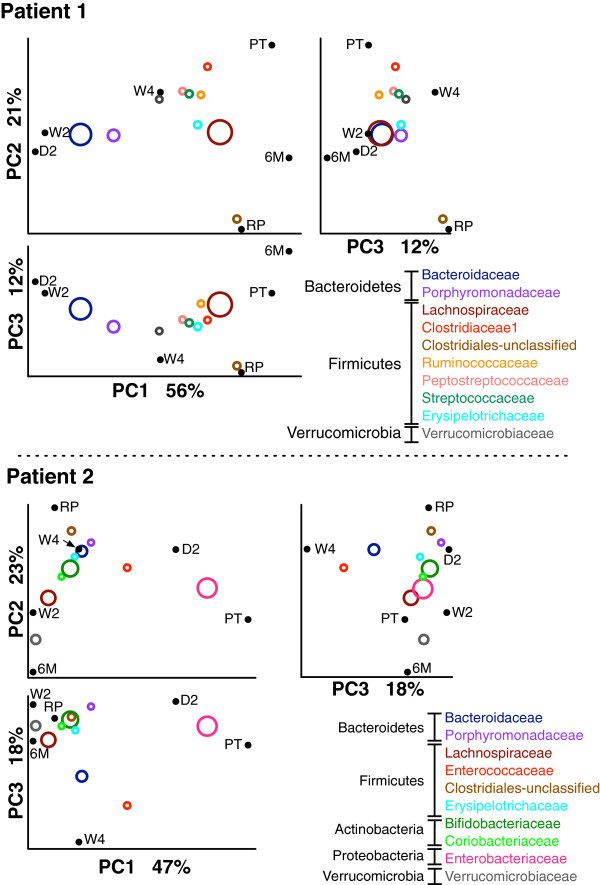
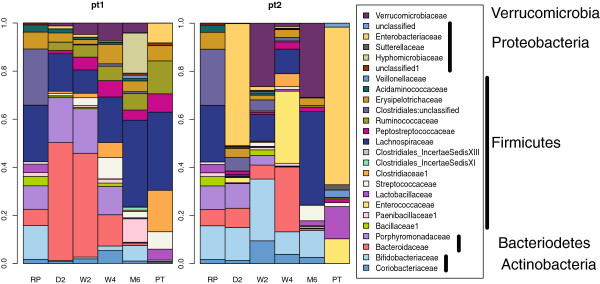
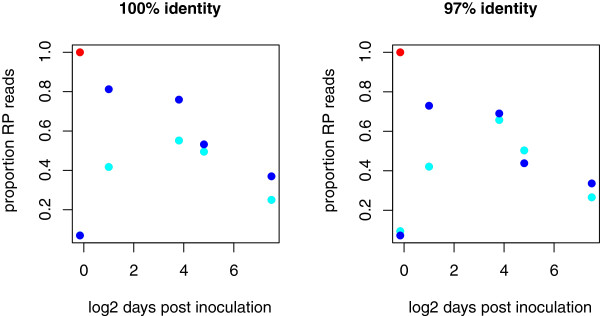
Results: Both patients were infected with the hyper virulent C. difficile strain, ribotype 078. Following stool substitute treatment, each patient reverted to their normal bowel pattern within 2 to 3 days and remained symptom-free at 6 months. The analysis demonstrated that rRNA sequences found in the stool substitute were rare in the pre-treatment stool samples but constituted over 25% of the sequences up to 6 months after treatment.
Conclusion: This proof-of-principle study demonstrates that a stool substitute mixture comprising a multi-species community of bacteria is capable of curing antibiotic-resistant C. difficile colitis. This benefit correlates with major changes in stool microbial profile and these changes reflect isolates from the synthetic mixture.
Clinical trial registration number: CinicalTrials.gov NCT01372943.
Figures
References
-
- Bartlett JG, Gerding DN. Clinical recognition and diagnosis of Clostridium difficile infection. Clin Infect Dis. 2008;46(Suppl 1):S12–S18. - PubMed
-
- Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG, McDonald LC, Pepin J, Wilcox MH. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the infectious diseases society of America (IDSA) Infect Control Hosp Epidemiol. 2010;31:431–455. doi: 10.1086/651706. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
