

Incremental prognostic value of coronary computed tomographic angiography over coronary artery calcium score for risk prediction of major adverse cardiac events in asymptomatic diabetic individuals
- PMID: 24468142
- PMCID: PMC4378659
- DOI: 10.1016/j.atherosclerosis.2013.09.025
Incremental prognostic value of coronary computed tomographic angiography over coronary artery calcium score for risk prediction of major adverse cardiac events in asymptomatic diabetic individuals
Abstract
Background: Coronary artery disease (CAD) diagnosis by coronary computed tomographic angiography (CCTA) is useful for identification of symptomatic diabetic individuals at heightened risk for death. Whether CCTA-detected CAD enables improved risk assessment of asymptomatic diabetic individuals beyond clinical risk factors and coronary artery calcium scoring (CACS) remains unexplored.
Methods: From a prospective 12-center international registry of 27,125 individuals undergoing CCTA, we identified 400 asymptomatic diabetic individuals without known CAD. Coronary stenosis by CCTA was graded as 0%, 1-49%, 50-69%, and ≥70%. CAD was judged on a per-patient, per-vessel and per-segment basis as maximal stenosis severity, number of vessels with ≥50% stenosis, and coronary segments weighted for stenosis severity (segment stenosis score), respectively. We assessed major adverse cardiovascular events (MACE) - inclusive of mortality, nonfatal myocardial infarction (MI), and late target vessel revascularization ≥90 days (REV) - and evaluated the incremental utility of CCTA for risk prediction, discrimination and reclassification.
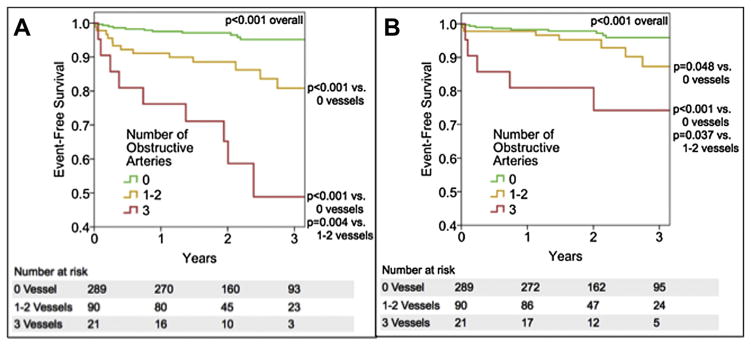
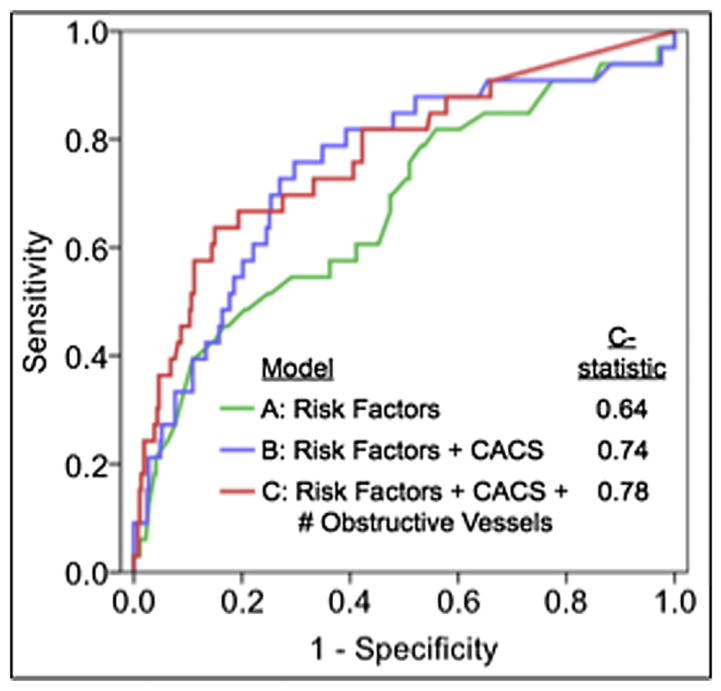
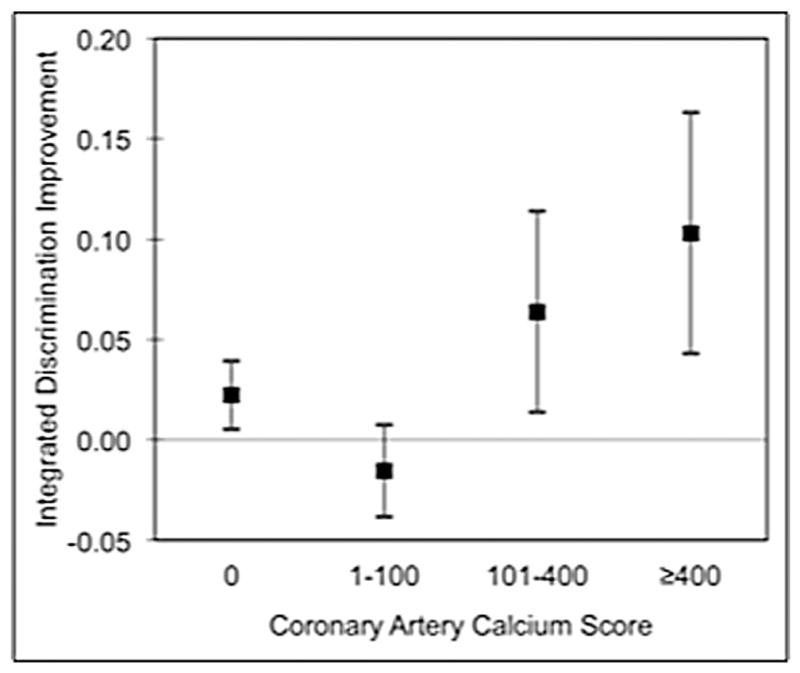
Results: Mean age was 60.4 ± 9.9 years; 65.0% were male. At a mean follow-up 2.4 ± 1.1 years, 33 MACE occurred (13 deaths, 8 MI, 12 REV) [8.25%; annualized rate 3.4%]. By univariate analysis, per-patient maximal stenosis [hazards ratio (HR) 2.24 per stenosis grade, 95% confidence interval (CI) 1.61-3.10, p < 0.001], increasing numbers of obstructive vessels (HR 2.30 per vessel, 95% CI 1.75-3.03, p < 0.001) and segment stenosis score (HR 1.14 per segment, 95% CI 1.09-1.19, p < 0.001) were associated with increased MACE. After adjustment for CAD risk factors and CACS, maximal stenosis (HR 1.80 per grade, 95% CI 1.18-2.75, p = 0.006), number of obstructive vessels (HR 1.85 per vessel, 95% CI 1.29-2.65, p < 0.001) and segment stenosis score (HR 1.11 per segment, 95% CI 1.05-1.18, p < 0.001) were associated with increased risk of MACE. Beyond age, gender and CACS (C-index 0.64), CCTA improved discrimination by maximal stenosis, number of obstructive vessels and segment stenosis score (C-index 0.77, 0.77 and 0.78, respectively). Similarly, CCTA findings improved risk reclassification by per-patient maximal stenosis [integrated discrimination improvement (IDI) index 0.03, p = 0.03] and number of obstructive vessels (IDI index 0.06, p = 0.002), and by trend for segment stenosis score (IDI 0.03, p = 0.06).
Conclusion: For asymptomatic diabetic individuals, CCTA measures of CAD severity confer incremental risk prediction, discrimination and reclassification on a per-patient, per-vessel and per-segment basis.
Keywords: Coronary CT angiography; Coronary artery calcium score; Coronary artery disease; Major adverse cardiac events.
Copyright © 2013 Elsevier Ireland Ltd. All rights reserved.
Figures
Similar articles
-
Incremental prognostic value of coronary computed tomography angiography over coronary calcium scoring for major adverse cardiac events in elderly asymptomatic individuals.Eur Heart J Cardiovasc Imaging. 2018 Jun 1;19(6):675-683. doi: 10.1093/ehjci/jex150. Eur Heart J Cardiovasc Imaging. 2018. PMID: 28977374 Free PMC article.
-
Does coronary CT angiography improve risk stratification over coronary calcium scoring in symptomatic patients with suspected coronary artery disease? Results from the prospective multicenter international CONFIRM registry.Eur Heart J Cardiovasc Imaging. 2014 Mar;15(3):267-74. doi: 10.1093/ehjci/jet148. Epub 2013 Aug 21. Eur Heart J Cardiovasc Imaging. 2014. PMID: 23966421
-
Age-related risk of major adverse cardiac event risk and coronary artery disease extent and severity by coronary CT angiography: results from 15 187 patients from the International Multisite CONFIRM Study.Eur Heart J Cardiovasc Imaging. 2014 May;15(5):586-94. doi: 10.1093/ehjci/jet132. Eur Heart J Cardiovasc Imaging. 2014. PMID: 24714312 Free PMC article.
-
Clinical Relevance of Coronary Computed Tomography Angiography Beyond Coronary Artery Stenosis.Rofo. 2021 Oct;193(10):1162-1170. doi: 10.1055/a-1395-7905. Epub 2021 Mar 26. Rofo. 2021. PMID: 33772488 Review. English.
-
Role of computed tomography for diagnosis and risk stratification of patients with suspected or known coronary artery disease.Arterioscler Thromb Vasc Biol. 2014 Jun;34(6):1144-54. doi: 10.1161/ATVBAHA.113.302074. Epub 2014 Apr 10. Arterioscler Thromb Vasc Biol. 2014. PMID: 24723554 Free PMC article. Review.
Cited by
-
State-of-the-Art Updates on Cardiac Computed Tomographic Angiography for Assessing Coronary Artery Disease.Curr Treat Options Cardiovasc Med. 2015 Aug;17(8):398. doi: 10.1007/s11936-015-0398-6. Curr Treat Options Cardiovasc Med. 2015. PMID: 26092612
-
Prediction of cardiovascular outcomes by imaging coronary atherosclerosis.Cardiovasc Diagn Ther. 2016 Aug;6(4):322-39. doi: 10.21037/cdt.2015.12.08. Cardiovasc Diagn Ther. 2016. PMID: 27500091 Free PMC article. Review.
-
High-risk coronary artery plaque in asymptomatic patients with type 2 diabetes: clinical risk factors and coronary artery calcium score.Cardiovasc Diabetol. 2021 Aug 9;20(1):164. doi: 10.1186/s12933-021-01350-2. Cardiovasc Diabetol. 2021. PMID: 34372839 Free PMC article.
-
Incremental prognostic value of coronary computed tomography angiography over coronary calcium scoring for major adverse cardiac events in elderly asymptomatic individuals.Eur Heart J Cardiovasc Imaging. 2018 Jun 1;19(6):675-683. doi: 10.1093/ehjci/jex150. Eur Heart J Cardiovasc Imaging. 2018. PMID: 28977374 Free PMC article.
-
Visual Coronary and Aortic Calcium Scoring on Chest Computed Tomography Predict Mortality in Patients With Low-Density Lipoprotein-Cholesterol ≥190 mg/dL.Circ Cardiovasc Imaging. 2022 Jun;15(6):e014135. doi: 10.1161/CIRCIMAGING.122.014135. Epub 2022 Jun 21. Circ Cardiovasc Imaging. 2022. PMID: 35727870 Free PMC article.
References
-
- Narayan KM, Boyle JP, Geiss LS, Saaddine JB, Thompson TJ. Impact of recent increase in incidence on future diabetes burden: U.S. 2005–2050. Diabetes Care. 2006;29:2114–6. - PubMed
-
- Third report of the National Cholesterol Education Program (NCEP) Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143–421. - PubMed
-
- Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: summary article. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines) J Am Coll Cardiol. 2002;40:1531–40. - PubMed
-
- Hendel RC, Berman DS, Di Carli MF, et al. ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 Appropriate use criteria for cardiac radionuclide imaging: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the American Society of Nuclear Cardiology, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the Society of Cardiovascular Computed Tomography, the Society for Cardiovascular Magnetic Resonance, and the Society of Nuclear Medicine. J Am Coll Cardiol. 2009;53:2201–29. - PubMed
-
- Taylor AJ, Cerqueira M, Hodgson JM, et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 Appropriate Use Criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. Circulation. 2010;122:e525–55. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
