

Incremental prognostic value of coronary computed tomographic angiography over coronary artery calcium score for risk prediction of major adverse cardiac events in asymptomatic diabetic individuals
- PMID: 24468142
- PMCID: PMC4378659
- DOI: 10.1016/j.atherosclerosis.2013.09.025
Incremental prognostic value of coronary computed tomographic angiography over coronary artery calcium score for risk prediction of major adverse cardiac events in asymptomatic diabetic individuals
Abstract
Background: Coronary artery disease (CAD) diagnosis by coronary computed tomographic angiography (CCTA) is useful for identification of symptomatic diabetic individuals at heightened risk for death. Whether CCTA-detected CAD enables improved risk assessment of asymptomatic diabetic individuals beyond clinical risk factors and coronary artery calcium scoring (CACS) remains unexplored.
Methods: From a prospective 12-center international registry of 27,125 individuals undergoing CCTA, we identified 400 asymptomatic diabetic individuals without known CAD. Coronary stenosis by CCTA was graded as 0%, 1-49%, 50-69%, and ≥70%. CAD was judged on a per-patient, per-vessel and per-segment basis as maximal stenosis severity, number of vessels with ≥50% stenosis, and coronary segments weighted for stenosis severity (segment stenosis score), respectively. We assessed major adverse cardiovascular events (MACE) - inclusive of mortality, nonfatal myocardial infarction (MI), and late target vessel revascularization ≥90 days (REV) - and evaluated the incremental utility of CCTA for risk prediction, discrimination and reclassification.
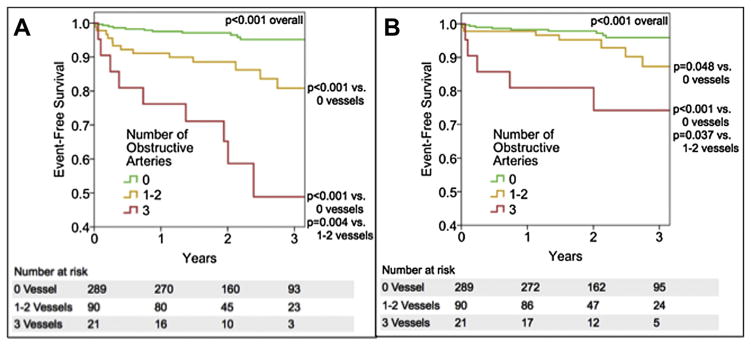
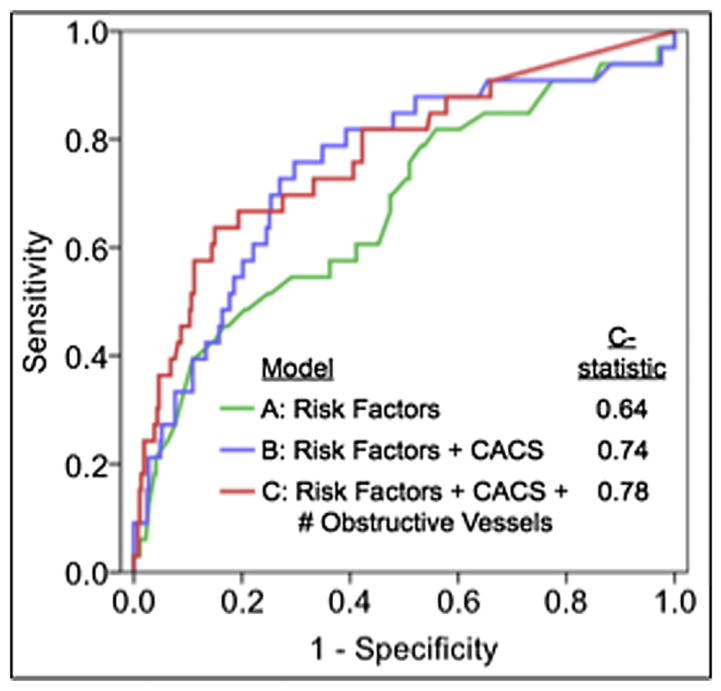
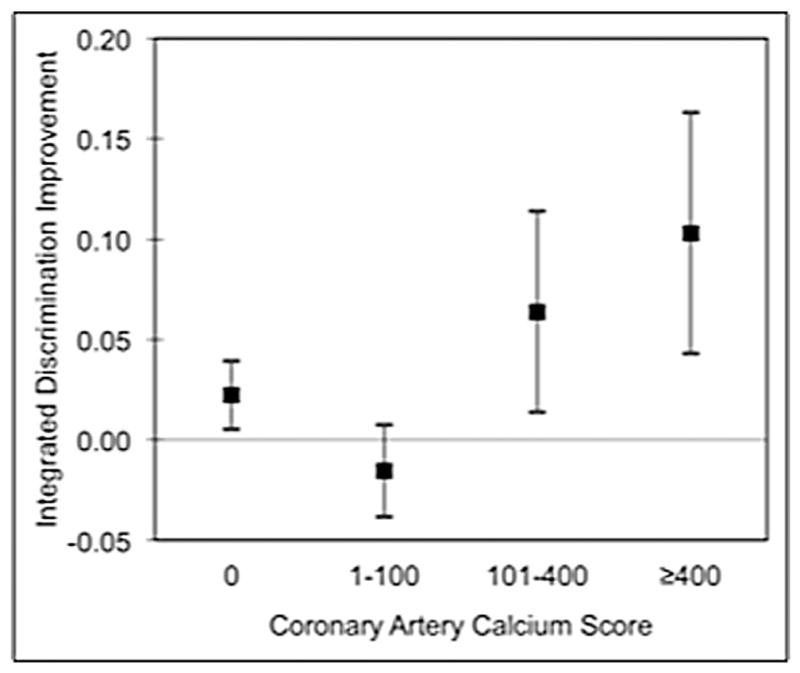
Results: Mean age was 60.4 ± 9.9 years; 65.0% were male. At a mean follow-up 2.4 ± 1.1 years, 33 MACE occurred (13 deaths, 8 MI, 12 REV) [8.25%; annualized rate 3.4%]. By univariate analysis, per-patient maximal stenosis [hazards ratio (HR) 2.24 per stenosis grade, 95% confidence interval (CI) 1.61-3.10, p < 0.001], increasing numbers of obstructive vessels (HR 2.30 per vessel, 95% CI 1.75-3.03, p < 0.001) and segment stenosis score (HR 1.14 per segment, 95% CI 1.09-1.19, p < 0.001) were associated with increased MACE. After adjustment for CAD risk factors and CACS, maximal stenosis (HR 1.80 per grade, 95% CI 1.18-2.75, p = 0.006), number of obstructive vessels (HR 1.85 per vessel, 95% CI 1.29-2.65, p < 0.001) and segment stenosis score (HR 1.11 per segment, 95% CI 1.05-1.18, p < 0.001) were associated with increased risk of MACE. Beyond age, gender and CACS (C-index 0.64), CCTA improved discrimination by maximal stenosis, number of obstructive vessels and segment stenosis score (C-index 0.77, 0.77 and 0.78, respectively). Similarly, CCTA findings improved risk reclassification by per-patient maximal stenosis [integrated discrimination improvement (IDI) index 0.03, p = 0.03] and number of obstructive vessels (IDI index 0.06, p = 0.002), and by trend for segment stenosis score (IDI 0.03, p = 0.06).
Conclusion: For asymptomatic diabetic individuals, CCTA measures of CAD severity confer incremental risk prediction, discrimination and reclassification on a per-patient, per-vessel and per-segment basis.
Keywords: Coronary CT angiography; Coronary artery calcium score; Coronary artery disease; Major adverse cardiac events.
Copyright © 2013 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- Narayan KM, Boyle JP, Geiss LS, Saaddine JB, Thompson TJ. Impact of recent increase in incidence on future diabetes burden: U.S. 2005–2050. Diabetes Care. 2006;29:2114–6. - PubMed
-
- Third report of the National Cholesterol Education Program (NCEP) Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143–421. - PubMed
-
- Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: summary article. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines) J Am Coll Cardiol. 2002;40:1531–40. - PubMed
-
- Hendel RC, Berman DS, Di Carli MF, et al. ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 Appropriate use criteria for cardiac radionuclide imaging: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the American Society of Nuclear Cardiology, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the Society of Cardiovascular Computed Tomography, the Society for Cardiovascular Magnetic Resonance, and the Society of Nuclear Medicine. J Am Coll Cardiol. 2009;53:2201–29. - PubMed
-
- Taylor AJ, Cerqueira M, Hodgson JM, et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 Appropriate Use Criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. Circulation. 2010;122:e525–55. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
