

Inverse association of colorectal cancer prevalence to serum levels of perfluorooctane sulfonate (PFOS) and perfluorooctanoate (PFOA) in a large Appalachian population
- PMID: 24468211
- PMCID: PMC3909456
- DOI: 10.1186/1471-2407-14-45
Inverse association of colorectal cancer prevalence to serum levels of perfluorooctane sulfonate (PFOS) and perfluorooctanoate (PFOA) in a large Appalachian population
Abstract
Background: Perfluorooctanoate (PFOA) and perfluorooctane sulfonate (PFOS) are persistent environmental contaminants that affect metabolic regulation, inflammation, and other factors implicated in the development and progression of colorectal cancer (CRC). However, the link between these compounds and CRC remains unknown. In this cross-sectional study, we investigated the association of CRC diagnosis to PFOA and PFOS blood levels in a large Appalachian population.
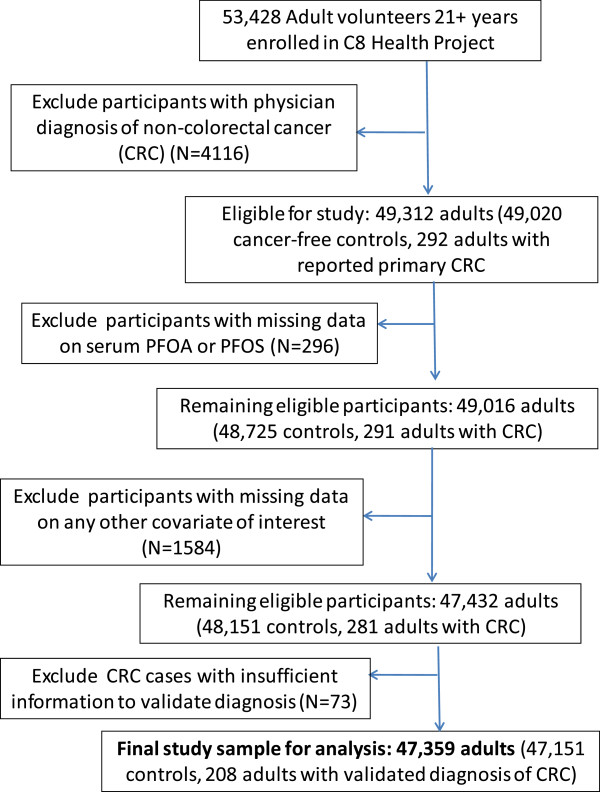
Methods: Participants were 47,359 adults ≥ 21 years of age and residing in six PFOA-contaminated water districts in the mid-Ohio Valley (N = 47,151 cancer-free adults, 208 cases of primary CRC). All participants completed a comprehensive health survey between 2005 and 2006; serum levels of PFOA, PFOS, and a range of other blood markers were also measured. Medical history was assessed via self report and cancer diagnosis confirmed via chart review.
Results: CRC showed a strong inverse, dose-response association with PFOS serum levels (odds ratio (OR) adjusted for potential confounders = 0.2, 95% confidence interval (CI) 0.2,0.3) for highest vs. lowest quartile of PFOS, P-trend < 0.00001) and a significant, but more modest inverse association with PFOA (adjusted OR = 0.6 (CI 0.4, 0.9) for highest vs. lowest quartile, P-trend = 0.001). These inverse associations were stronger in those diagnosed within the previous 6 years and resident in the same water district for a minimum of 10-15 years preceding assessment. The relationship between PFOA and CRC was also more pronounced in men and leaner adults, and showed a stronger linear trend at lower exposure levels.
Conclusions: In this large cross-sectional study, we found a strong, inverse association between PFOS and likelihood of CRC diagnosis and a significant, although more modest inverse association between PFOA and CRC. If confirmed in prospective investigations, these findings may aid in identifying new strategies for CRC prevention and treatment and inform future studies regarding mechanisms underlying CRC pathogenesis.
Figures

References
-
- U.S. Cancer Statistics Working Group, United States Cancer Statistics. 1999–2006 Incidence and Mortality Web-based Report. Atlanta (GA): Department of Health and Human Services, Centers for Disease Control and Prevention, and National Cancer Institute; 2010.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
