

How do different eligibility guidelines for antiretroviral therapy affect the cost-effectiveness of routine viral load testing in sub-Saharan Africa?
- PMID: 24468949
- PMCID: PMC4089870
- DOI: 10.1097/QAD.0000000000000110
How do different eligibility guidelines for antiretroviral therapy affect the cost-effectiveness of routine viral load testing in sub-Saharan Africa?
Abstract
Background: Increased eligibility guidelines of antiretroviral therapy (ART) may lead to greater routine viral load monitoring. However, in resource-constrained settings, the additional resources required by greater routine viral load monitoring may impair ability to comply with expanded eligibility guidelines for ART.
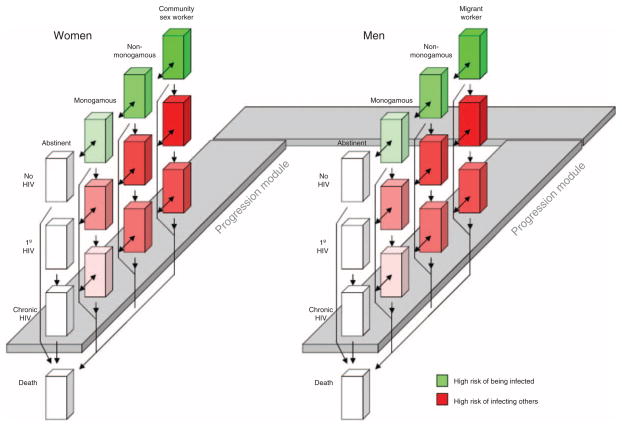
Objective: We use a published validated computer simulation of the HIV epidemic in East African countries (expanded to include transmission as well as disease progression) to evaluate the cost-effectiveness of routine viral load monitoring.
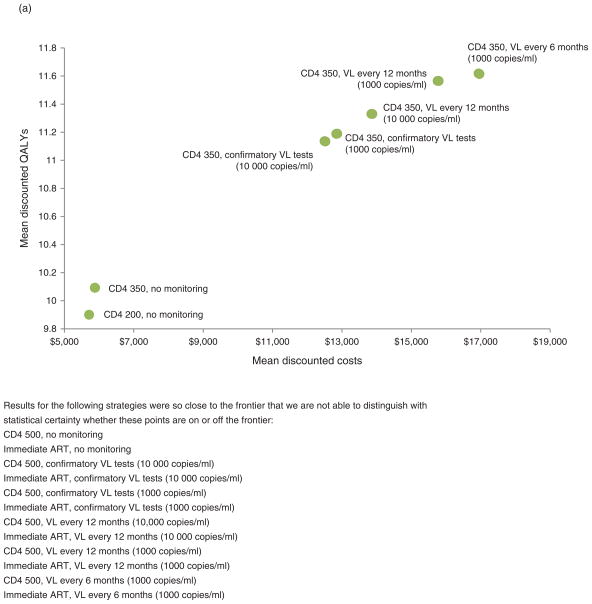
Methods: We explored alternative scenarios regarding cost, frequency, and switching threshold of routine viral load monitoring (including every 6 or every 12 months; and switching thresholds of 1000, or 10 000 copies/ml), as well as alternative scenarios regarding ART initiation (200, 350, 500 cells/μl, and no CD4 cell threshold). For each ART initiation strategy, we sought to identify the viral load monitoring strategy at which the incremental cost-effectiveness ratio (ICER) of more frequent routine viral load testing became more favorable than the ICER of more expansive ART eligibility. Cost inputs were based on data provided by the Academic Model Providing Access to Healthcare (AMPATH), and disease progression inputs were based on prior published work. We used a discount rate of 3%, a time horizon of 20 years, and a payer perspective.
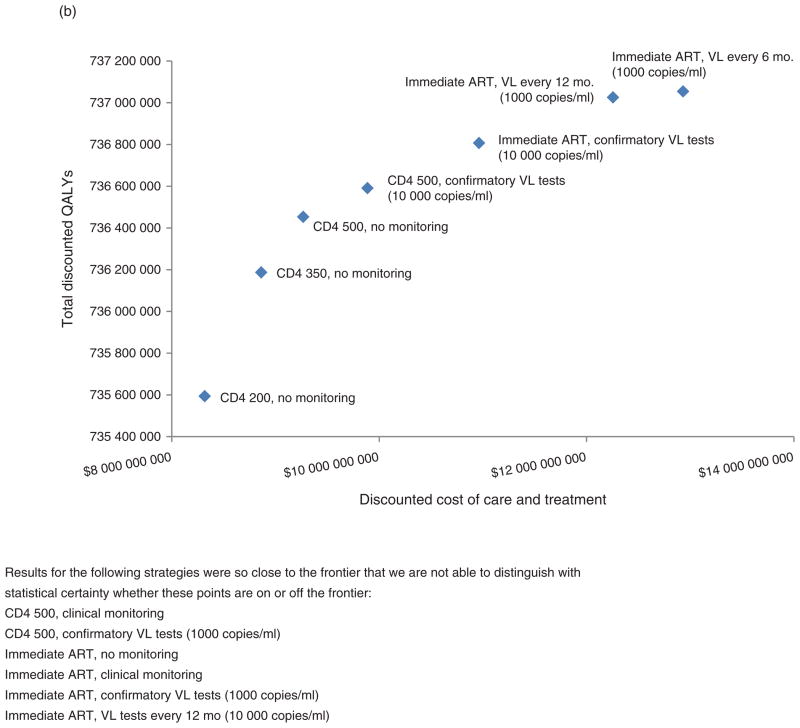
Results: Across a wide range of scenarios, and even when considering the beneficial effect of virological monitoring at reducing HIV transmission, earlier ART initiation conferred far greater health benefits for resources spent than routine virological testing, with ICERs of approximately $1000 to $2000 for earlier ART initiation, versus ICERs of approximately $5000 to $25 000 for routine virological monitoring. ICERs of viral load testing were insensitive to the cost of the viral load test, because most of the costs originated from the downstream higher costs of later regimens. ICERs of viral load testing were very sensitive to the relative cost of second-line compared with first-line regimens, assuming favorable value when the costs of these regimens were equal.
Conclusion: If all HIV patients are not yet treated with ART starting at 500 cells/μl and costs of second regimens remain substantially more expensive than first-line regimens, resources would buy more population health if they are spent on earlier ART rather than being spent on routine virological testing.
Conflict of interest statement
None.
Figures
Similar articles
-
Monitoring and switching of first-line antiretroviral therapy in adult treatment cohorts in sub-Saharan Africa: collaborative analysis.Lancet HIV. 2015 Jul;2(7):e271-8. doi: 10.1016/S2352-3018(15)00087-9. Epub 2015 Jun 16. Lancet HIV. 2015. PMID: 26423252 Free PMC article.
-
CD4 cell count and viral load monitoring in patients undergoing antiretroviral therapy in Uganda: cost effectiveness study.BMJ. 2011 Nov 9;343:d6884. doi: 10.1136/bmj.d6884. BMJ. 2011. PMID: 22074713 Free PMC article. Clinical Trial.
-
Extraordinary heterogeneity of virological outcomes in patients receiving highly antiretroviral therapy and monitored with the World Health Organization public health approach in sub-saharan Africa and southeast Asia.Clin Infect Dis. 2014 Jan;58(1):99-109. doi: 10.1093/cid/cit627. Epub 2013 Sep 27. Clin Infect Dis. 2014. PMID: 24076968
-
Modeling the cost-effectiveness of HIV treatment: how to buy the most 'health' when resources are limited.Curr Opin HIV AIDS. 2013 Nov;8(6):544-9. doi: 10.1097/COH.0000000000000005. Curr Opin HIV AIDS. 2013. PMID: 24100874 Free PMC article. Review.
-
Economic evaluation of ART in resource-limited countries.Curr Opin HIV AIDS. 2010 May;5(3):225-31. doi: 10.1097/COH.0b013e3283384a9d. Curr Opin HIV AIDS. 2010. PMID: 20539078 Free PMC article. Review.
Cited by
-
Optimal timing of viral load monitoring during pregnancy to predict viraemia at delivery in HIV-infected women initiating ART in South Africa: a simulation study.J Int AIDS Soc. 2017 Nov;20 Suppl 7(Suppl 7):e25000. doi: 10.1002/jia2.25000. J Int AIDS Soc. 2017. PMID: 29171179 Free PMC article.
-
Choice of time horizon critical in estimating costs and effects of changes to HIV programmes.PLoS One. 2018 May 16;13(5):e0196480. doi: 10.1371/journal.pone.0196480. eCollection 2018. PLoS One. 2018. PMID: 29768457 Free PMC article.
-
Universal test, treat, and keep: improving ART retention is key in cost-effective HIV control in Uganda.BMC Infect Dis. 2017 May 3;17(1):322. doi: 10.1186/s12879-017-2420-y. BMC Infect Dis. 2017. PMID: 28468605 Free PMC article.
-
Targeting an alcohol intervention cost-effectively to persons living with HIV/AIDS in East Africa.Alcohol Clin Exp Res. 2015 Nov;39(11):2179-88. doi: 10.1111/acer.12890. Epub 2015 Oct 14. Alcohol Clin Exp Res. 2015. PMID: 26463727 Free PMC article.
-
Clinical Benefits and Cost-Effectiveness of Laboratory Monitoring Strategies to Guide Antiretroviral Treatment Switching in India.AIDS Res Hum Retroviruses. 2018 Jun;34(6):486-497. doi: 10.1089/AID.2017.0258. Epub 2018 May 3. AIDS Res Hum Retroviruses. 2018. PMID: 29620932 Free PMC article.
References
-
- World Health Organization. Antiretroviral therapy for HIV infection in adults and adolescents: recommendations for a public health approach. 2010 revision. - PubMed
-
- Markowitz H. Portfolio selection. J Finance. 1952;53:405–411.
-
- Bajunirwe F, Arts EJ, Tisch DJ, King CH, Debanne SM, Sethi AK. Adherence and treatment response among HIV-1-infected adults receiving antiretroviral therapy in a rural government hospital in southwestern Uganda. J Int Assoc Physicians AIDS Care (Chic) 2009;8:139–147. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
