

Retention in care under universal antiretroviral therapy for HIV-infected pregnant and breastfeeding women ('Option B+') in Malawi
- PMID: 24468999
- PMCID: PMC4009400
- DOI: 10.1097/QAD.0000000000000143
Retention in care under universal antiretroviral therapy for HIV-infected pregnant and breastfeeding women ('Option B+') in Malawi
Abstract
Objective: To explore the levels and determinants of loss to follow-up (LTF) under universal lifelong antiretroviral therapy (ART) for pregnant and breastfeeding women ('Option B+') in Malawi.
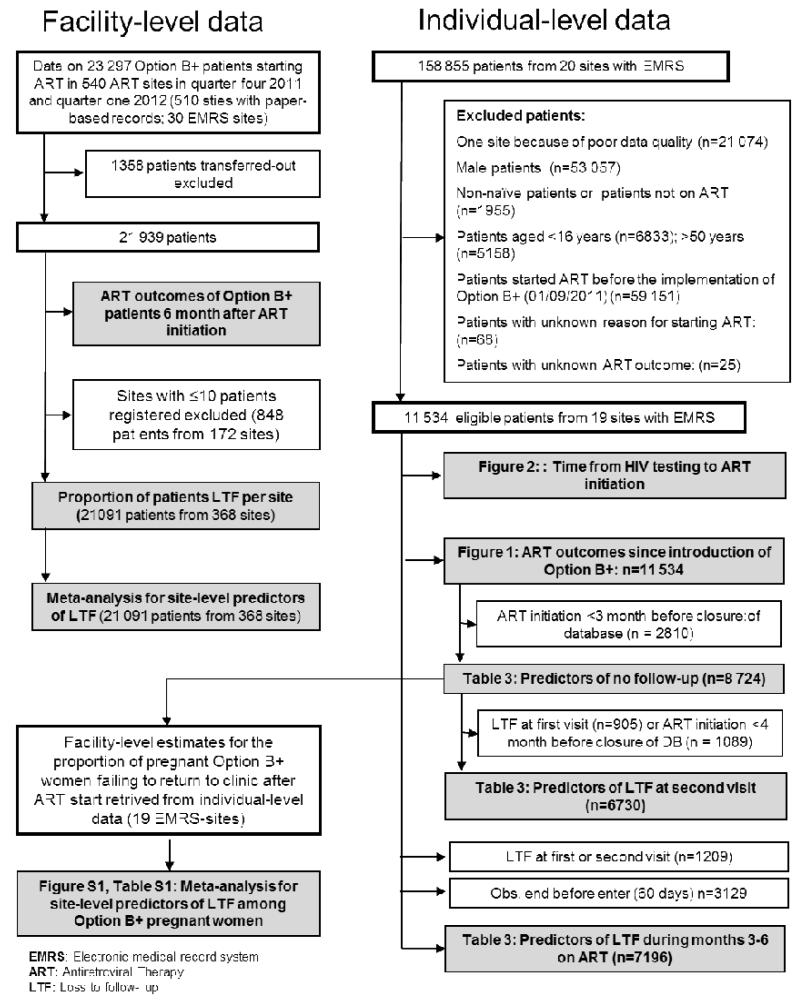
Design, setting, and participants: We examined retention in care, from the date of ART initiation up to 6 months, for women in the Option B+ program. We analysed nationwide facility-level data on women who started ART at 540 facilities (n = 21,939), as well as individual-level data on patients who started ART at 19 large facilities (n = 11,534).
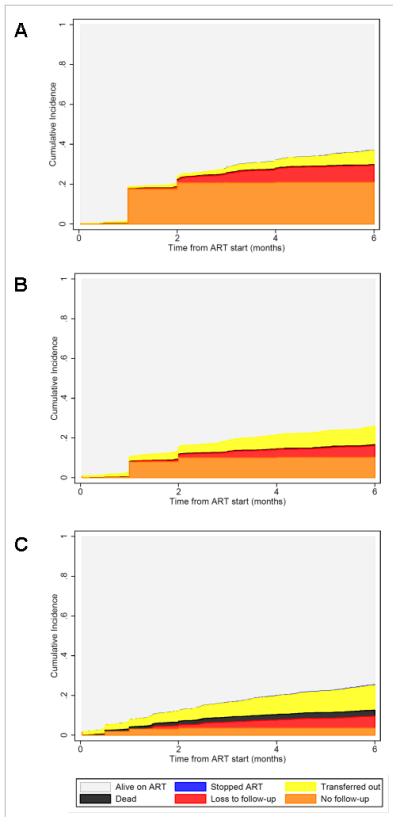
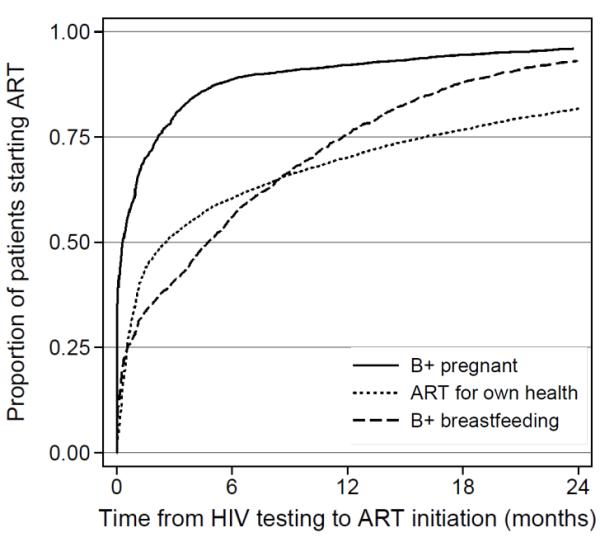
Results: Of the women who started ART under Option B+ (n = 21,939), 17% appeared to be lost to follow-up 6 months after ART initiation. Most losses occurred in the first 3 months of therapy. Option B+ patients who started therapy during pregnancy were five times more likely than women who started ART in WHO stage 3/4 or with a CD4 cell count 350 cells/μl or less, to never return after their initial clinic visit [odds ratio (OR) 5.0, 95% confidence interval (CI) 4.2-6.1]. Option B+ patients who started therapy while breastfeeding were twice as likely to miss their first follow-up visit (OR 2.2, 95% CI 1.8-2.8). LTF was highest in pregnant Option B+ patients who began ART at large clinics on the day they were diagnosed with HIV. LTF varied considerably between facilities, ranging from 0 to 58%.
Conclusion: Decreasing LTF will improve the effectiveness of the Option B+ approach. Tailored interventions, like community or family-based models of care could improve its effectiveness.
Figures
Comment in
-
Option B+ for prevention of mother-to-child transmission of HIV in resource-constrained settings: great promise but some early caution.AIDS. 2014 Feb 20;28(4):599-601. doi: 10.1097/QAD.0000000000000144. AIDS. 2014. PMID: 24469000 No abstract available.
References
-
- World Health Organisation [Accessed 1.5.2013];PMTCT strategic vision 2010-2015. Preventing mother-to-child transmission of HIV to reach the UNGASS and Millennium Development Goals 2010. Available at http://www.who.int/hiv/pub/mtct/strategic_vision/en/
-
- World Health Organisation [Accessed 1.5.2013];Antiretroviral drugs for treating pregnant women and preventing HIV infection in infants. Recommendations for a public health approach 2010 revision. Available at http://whqlibdoc.who.int/publications/2010/9789241599818_eng.pdf. - PubMed
-
- Mofenson L. Prevention in neglected subpopulations: prevention of mother-to-child transmission of HIV infection. Clin Infect Dis. 2010;50(Suppl 3):130–148. - PubMed
-
- Schouten EJ, Jahn A, Chimbwandira F, Harries AD, Van Damme W. Is Option B+ the best choice? Lancet. 2013 Apr 13;381(9874):1272–3. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
