

Pregnant women living with HIV (WLH) supported at clinics by peer WLH: a cluster randomized controlled trial
- PMID: 24469222
- PMCID: PMC4109271
- DOI: 10.1007/s10461-014-0694-2
Pregnant women living with HIV (WLH) supported at clinics by peer WLH: a cluster randomized controlled trial
Abstract
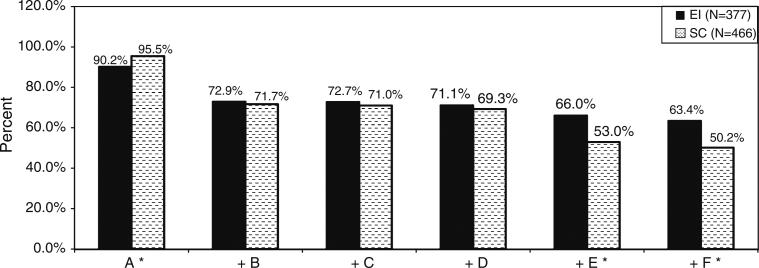
Throughout Africa, Peer Mentors who are women living with HIV (WLH) are supporting pregnant WLH at antenatal and primary healthcare clinics (McColl in BMJ 344:e1590, 2012). We evaluate a program using this intervention strategy at 1.5 months post-birth. In a cluster randomized controlled trial in KwaZulu-Natal, South Africa, eight clinics were randomized for their WLH to receive either: standard care (SC), based on national guidelines to prevent mother-to-child transmission (4 clinics; n = 656 WLH); or an enhanced intervention (EI; 4 clinics; n = 544 WLH). The EI consisted of four antenatal and four postnatal small group sessions led by Peer Mentors, in addition to SC. WLH were recruited during pregnancy and 70 % were reassessed at 1.5 months post-birth. EI's effect was ascertained on 16 measures of maternal and infant well-being using random effects regressions to control for clinic clustering. A binomial test for correlated outcomes evaluated EI's overall effectiveness. Among EI WLH reassessed, 87 % attended at least one intervention session (mean 4.1, SD 2.0). Significant overall benefits were found in EI compared to SC using the binomial test. However, it is important to note that EI WLH were significantly less likely to adhere to ARV during pregnancy compared to SC. Secondarily, compared to SC, EI WLH were more likely to ask partners to test for HIV, better protected their infants from HIV transmission, and were less likely to have depressed mood and stunted infants. Adherence to clinic intervention groups was low, yet, there were benefits for maternal and infant health at 1.5 months post-birth.
Trial registration: ClinicalTrials.gov NCT00972699.
Figures

References
-
- McColl K. Mentor mothers to prevent mother-to-child transmission of HIV. BMJ. 2012;344:e1590. - PubMed
-
- UNICEF [20 Feb 2013];Children and AIDS: Fourth Stocktaking Report. 2009 Available at: http://www.unicef.org/publications/files/Children_and_AIDS_Fourth_Stockt....
-
- AVERTing HIV and AIDS [20 Feb 2013];Sub-Saharan Africa HIV & AIDS Statistics. 2009 Available at: http://www.avert.org/africa-hiv-aids-statistics.htm.
-
- Shisana O, Rehle T, Simbayi LC, Zuma K, Jooste S, Pillay-van-Wyk V, et al. South African national HIV prevalence, incidence, behaviour and communication survey 2008: a turning tide among teenagers? HSRC Press; Cape Town: 2009.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
