

Observations from the IMPROVE trial concerning the clinical care of patients with ruptured abdominal aortic aneurysm
- PMID: 24469620
- PMCID: PMC4164272
- DOI: 10.1002/bjs.9410
Observations from the IMPROVE trial concerning the clinical care of patients with ruptured abdominal aortic aneurysm
Abstract
Background: Single-centre series of the management of patients with ruptured abdominal aortic aneurysm (AAA) are usually too small to identify clinical factors that could improve patient outcomes.
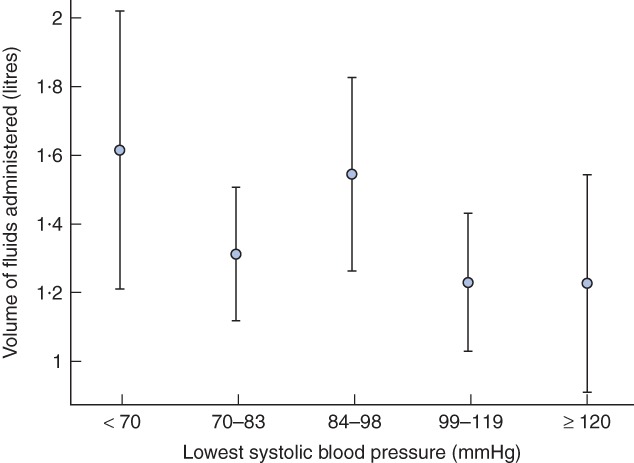
Methods: IMPROVE is a pragmatic, multicentre randomized clinical trial in which eligible patients with a clinical diagnosis of ruptured aneurysm were allocated to a strategy of endovascular aneurysm repair (EVAR) or to open repair. The influences of time and manner of hospital presentation, fluid volume status, type of anaesthesia, type of endovascular repair and time to aneurysm repair on 30-day mortality were investigated according to a prespecified plan, for the subgroup of patients with a proven diagnosis of ruptured or symptomatic AAA. Adjustment was made for potential confounding factors.
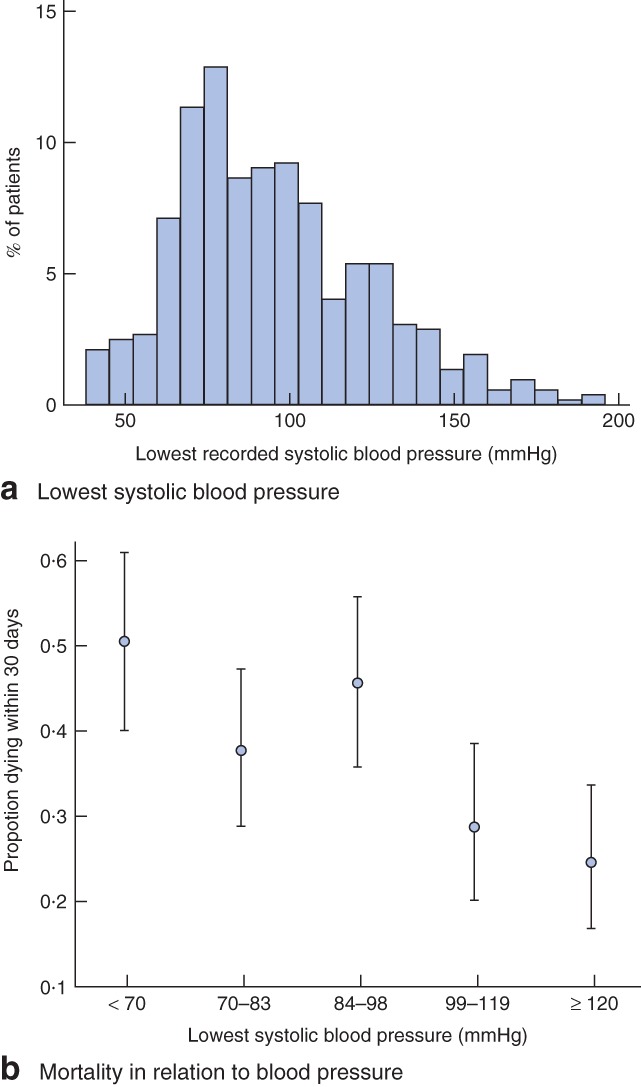
Results: Some 558 of 613 randomized patients had a symptomatic or ruptured aneurysm: diagnostic accuracy was 91·0 per cent. Patients randomized outside routine working hours had higher operative mortality (adjusted odds ratio (OR) 1·47, 95 per cent confidence interval 1·00 to 2·17). Mortality rates after primary and secondary presentation were similar. Lowest systolic blood pressure was strongly and independently associated with 30-day mortality (51 per cent among those with pressure below 70 mmHg). Patients who received EVAR under local anaesthesia alone had greatly reduced 30-day mortality compared with those who had general anaesthesia (adjusted OR 0·27, 0·10 to 0·70).
Conclusion: These findings suggest that the outcome of ruptured AAA might be improved by wider use of local anaesthesia for EVAR and that a minimum blood pressure of 70 mmHg is too low a threshold for permissive hypotension.
© 2014 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
References
-
- Holt PJ, Poloniecki JD, Gerrard D, Loftus IM, Thompson MM. Meta-analysis and systematic review of the relationship between volume and outcome in abdominal aortic aneurysm surgery. Br J Surg. 2007;94:395–403. - PubMed
-
- Symons NR, Moorthy K, Almoudaris AM, Bottle A, Aylin P, Vincent CA, et al. Mortality in high-risk emergency general surgical admissions. Br J Surg. 2013;100:1318–1325. - PubMed
-
- Mayer D, Aeschbacher S, Pfammatter T, Veith FJ, Norgren L, Magnuson A, et al. Complete replacement of open repair for ruptured abdominal aortic aneurysms by endovascular aneurysm repair: a two-center 14-year experience. Ann Surg. 2012;256:688–695. - PubMed
-
- Reimerink JJ, Hoornweg LL, Vahl AC, Wisselink W, van den Broek TA, Legemate DA, et al. Amsterdan Acute Aneurysm Trial Collaborators. Endovascular repair versus open repair of ruptured abdominal aortic aneurysms: a multicenter randomized controlled trial. Ann Surg. 2013;258:248–256. - PubMed
-
- Imperial College London. Immediate Management of Patients with Ruptured aneurysm: Open Versus Endovascular Repair (IMPROVE) http://www.imperial.ac.uk/medicine/improvetrial [accessed 1 October 2013]
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
