

Modulation of the relationship between external knee adduction moments and medial joint contact forces across subjects and activities
- PMID: 24470261
- PMCID: PMC4158863
- DOI: 10.1002/art.38374
Modulation of the relationship between external knee adduction moments and medial joint contact forces across subjects and activities
Abstract
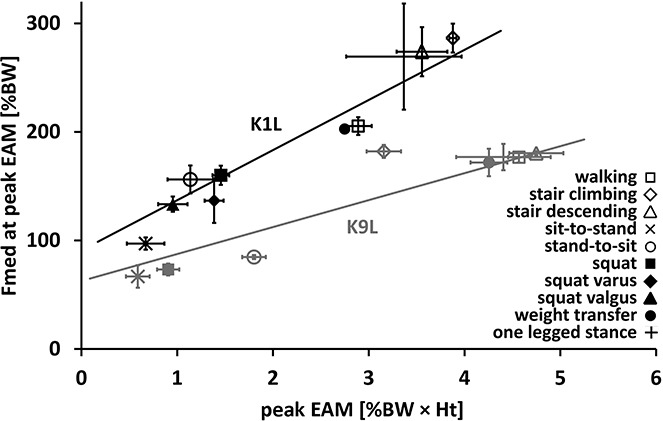
Objective: The external knee adduction moment (EAM) is often considered a surrogate measure of the distribution of loads across the tibiofemoral joint during walking. This study was undertaken to quantify the relationship between the EAM and directly measured medial tibiofemoral contact forces (Fmed ) in a sample of subjects across a spectrum of activities.
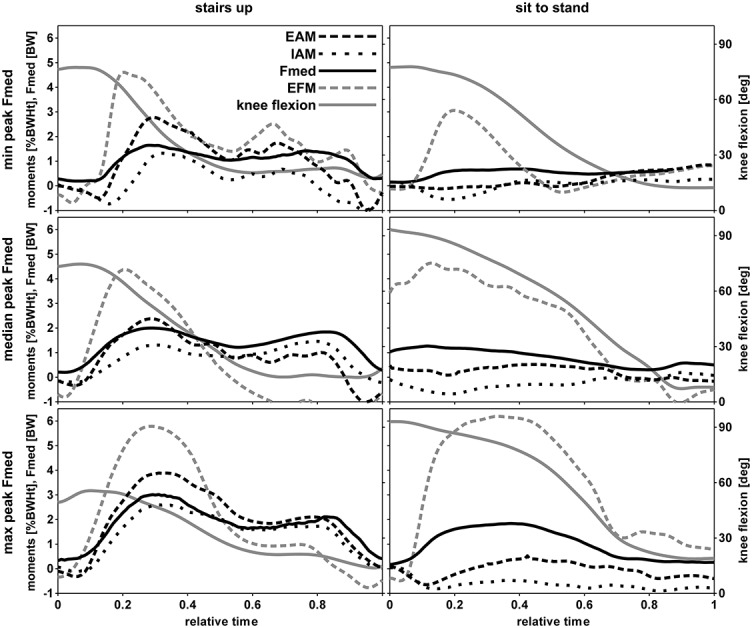
Methods: The EAM for 9 patients who underwent total knee replacement was calculated using inverse dynamics analysis, while telemetric implants provided Fmed for multiple repetitions of 10 activities, including walking, stair negotiation, sit-to-stand activities, and squatting. The effects of the factors "subject" and "activity" on the relationships between Fmed and EAM were quantified using mixed-effects regression analyses in terms of the root mean square error (RMSE) and the slope of the regression.
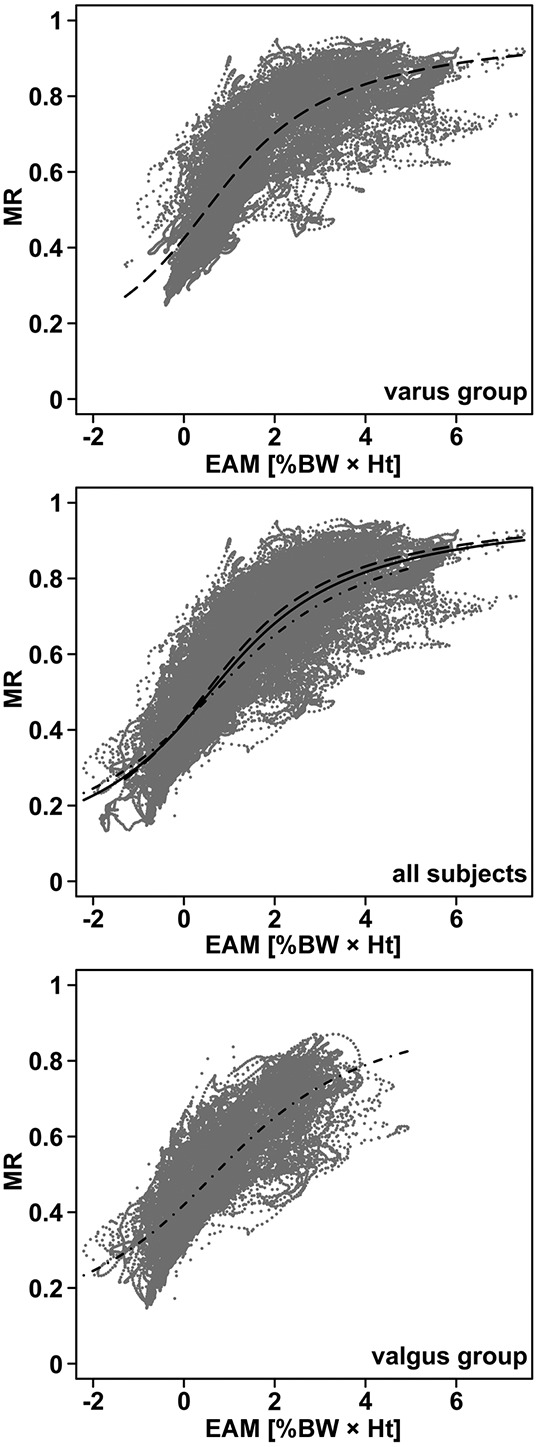
Results: Across subjects and activities a good correlation between peak EAM and Fmed values was observed, with an overall R(2) value of 0.88. However, the slope of the linear regressions varied between subjects by up to a factor of 2. At peak EAM and Fmed , the RMSE of the regression across all subjects was 35% body weight (%BW), while the maximum error was 127 %BW.
Conclusion: The relationship between EAM and Fmed is generally good but varies considerably across subjects and activities. These findings emphasize the limitation of relying solely on the EAM to infer medial joint loading when excessive directed cocontraction of muscles exists and call for further investigations into the soft tissue-related mechanisms that modulate the internal forces at the knee.
Copyright © 2014 by the American College of Rheumatology.
Figures
References
-
- D'Lima DD, Patil S, Steklov N, Slamin JE, Colwell CW., Jr Tibial forces measured in vivo after total knee arthroplasty. J Arthroplasty. 2006;21:255–62. - PubMed
-
- Kutzner I, Heinlein B, Graichen F, Bender A, Rohlmann A, Halder A, et al. Loading of the knee joint during activities of daily living measured in vivo in five subjects. J Biomech. 2010;43:2164–73. - PubMed
-
- Dieppe PA, Lohmander LS. Pathogenesis and management of pain in osteoarthritis. Lancet. 2005;365:965–73. - PubMed
-
- Prodromos CC, Andriacchi TP, Galante JO. A relationship between gait and clinical changes following high tibial osteotomy. J Bone Joint Surg Am. 1985;67:1188–94. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
