

An analysis of the learning curve to achieve competency at colonoscopy using the JETS database
- PMID: 24470280
- PMCID: PMC4215302
- DOI: 10.1136/gutjnl-2013-305973
An analysis of the learning curve to achieve competency at colonoscopy using the JETS database
Abstract
Objective: The number of colonoscopies required to reach competency is not well established. The primary aim of this study was to determine the number of colonoscopies trainees need to perform to attain competency, defined by a caecal intubation rate (CIR) ≥90%. As competency depends on completion, we also investigated trainee factors that were associated with colonoscopy completion.
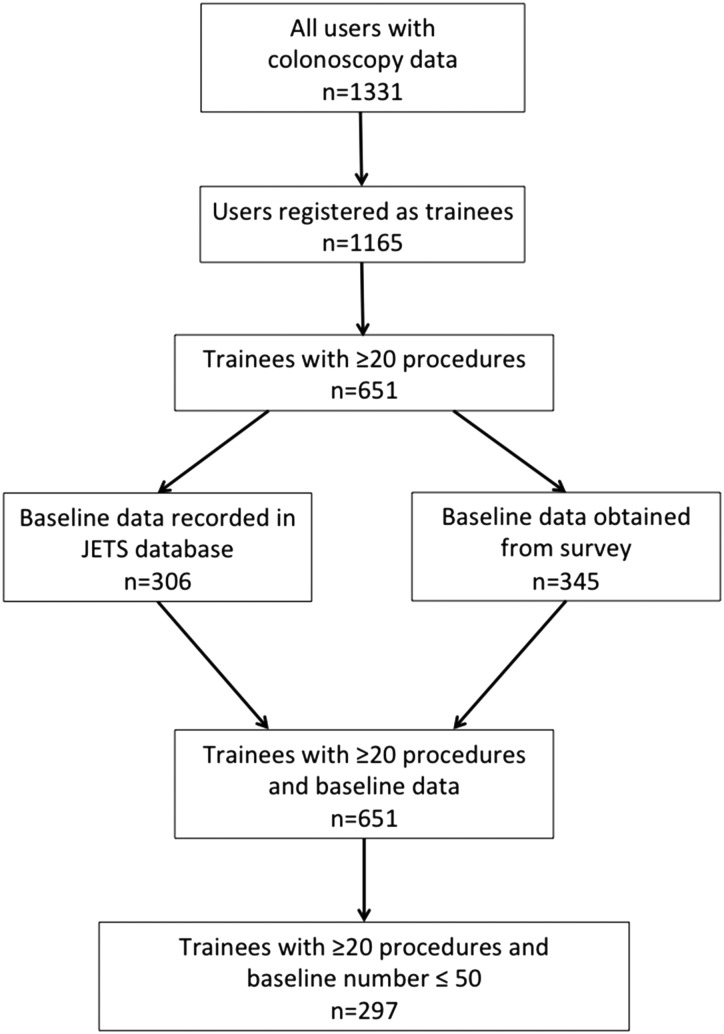
Design: The Joint Advisory Group on GI Endoscopy in the UK has developed a trainee e-portfolio from which colonoscopy data were retrieved. Inclusion criteria were all trainees who had performed a total of ≥20 colonoscopies and had performed ≤50 colonoscopies prior to submission of data to the e-portfolio. The primary outcome measure was colonoscopy completion. The number of colonoscopies required to achieve CIR ≥90% was calculated by the moving average method and learning curve cumulative summation (LC-Cusum) analysis. To determine factors which determine colonoscopy completion, a mixed effect logistic regression model was developed which allowed for nesting of patients within trainees and nesting of patients within hospitals, with various patient, trainee and training factors entered as fixed effects.
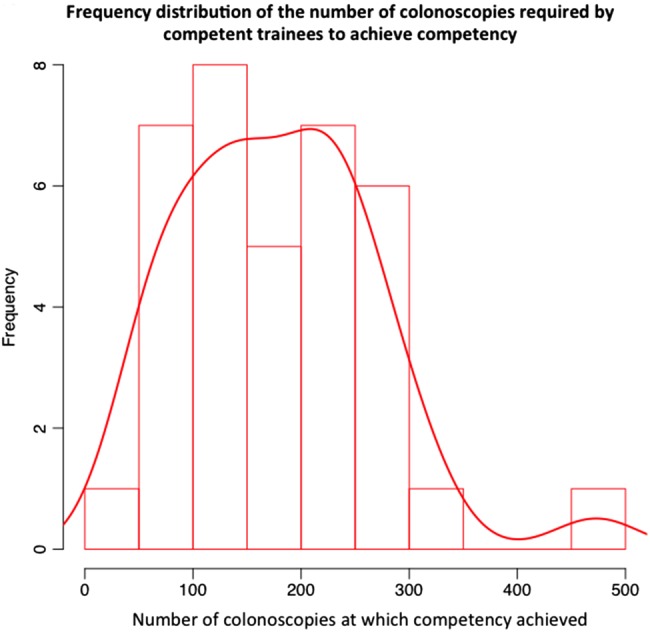
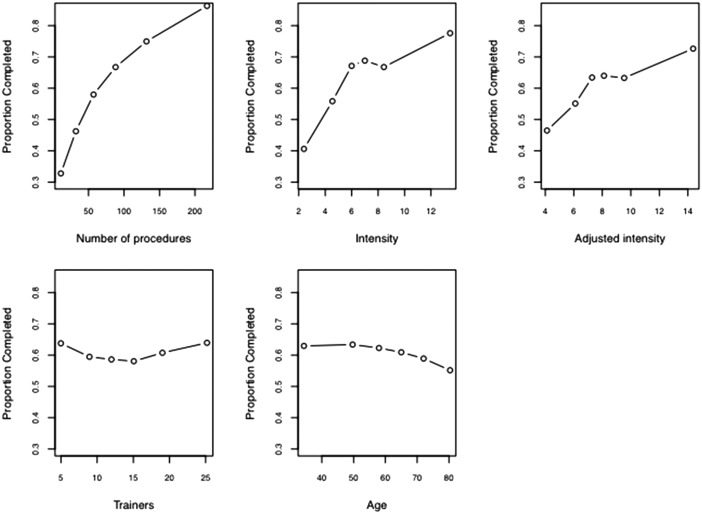
Results: 297 trainees undertook 36 730 colonoscopies. By moving average analysis, the cohort of trainees reached a CIR of 90% at 233 procedures. By LC-Cusum analysis, 41% of trainees were competent after 200 procedures. Of the trainee factors, the number of colonoscopies, intensity of training and previous flexible sigmoidoscopy experience were significant factors associated with colonoscopy completion.
Conclusions: This is the largest study to date investigating the number of procedures required to achieve competency in colonoscopy. The current training certification benchmark in the UK of 200 procedures does not appear to be an inappropriate minimum requirement. The LC-Cusum chart provides real time feedback on individual learning curves for trainees. The association of training intensity and flexible sigmoidoscopy experience with colonoscopy completion could be exploited in training programmes.
Keywords: Colonoscopy.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures

Comment in
-
Endoscopy training: time to stop counting procedures?Gut. 2014 Nov;63(11):1686-7. doi: 10.1136/gutjnl-2014-306765. Epub 2014 Mar 6. Gut. 2014. PMID: 24604824 No abstract available.
-
Caecal intubation rates and colonoscopy competency.Gut. 2015 Feb;64(2):359. doi: 10.1136/gutjnl-2014-307242. Epub 2014 Apr 9. Gut. 2015. PMID: 24717933 No abstract available.
-
Training the competent colonoscopist.Gastroenterology. 2014 Sep;147(3):708-9. doi: 10.1053/j.gastro.2014.07.009. Epub 2014 Jul 21. Gastroenterology. 2014. PMID: 25058019 No abstract available.
References
-
- NHS Cancer Screening Programmes, Great Britain, National Health Service. Quality assurance guidelines for colonoscopy. Sheffield: NHS Cancer Screening Programmes, 2011.
-
- Rex DK, Bond JH, Winawer S, et al. Quality in the technical performance of colonoscopy and the continuous quality improvement process for colonoscopy: recommendations of the U.S. Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol 2002;97:1296–308. - PubMed
-
- JAG Joint Advisory Group on GI Endoscopy. BSG Quality and Safety Indicators for Endoscopy. http://www.thejag.org.uk/downloads%5CUnit%20Resources%5CBSG%20Quality%20... (accessed 7 Jan 2013).
-
- Johna S, Klaristenfeld D. Surgery resident training in endoscopy: the saga continues. Arch Surg 2011;146:899–900. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials