

Analysis of IDH mutation, 1p/19q deletion, and PTEN loss delineates prognosis in clinical low-grade diffuse gliomas
- PMID: 24470545
- PMCID: PMC4057130
- DOI: 10.1093/neuonc/not299
Analysis of IDH mutation, 1p/19q deletion, and PTEN loss delineates prognosis in clinical low-grade diffuse gliomas
Abstract
Background: Grades II and III gliomas have unpredictable rates of progression, making management decisions difficult. Currently, several clinical and radiological characteristics are utilized to predict progression and survival but collectively are suboptimal.
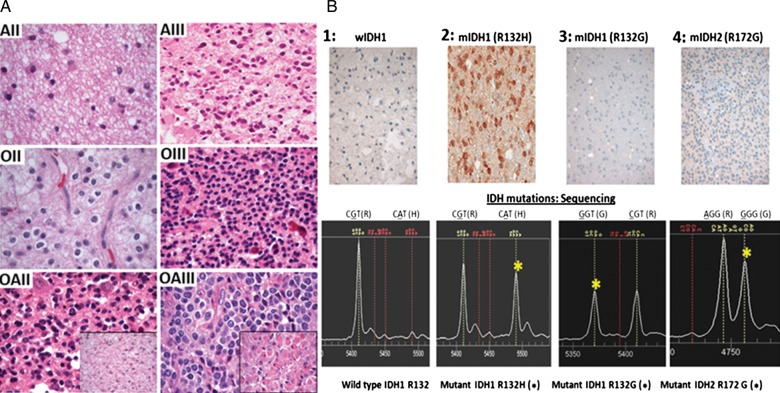
Methods: In this study, we analyzed a set of 108 nonenhancing hemispheric grade II-III gliomas. Demographic variables, including patient age, tumor diameter, extent of resection, and performance status, were combined with molecular data (IDH mutation status [mIDH], 1p/19q codeletion, PTEN deletion, and EGFR amplification). A complete dataset for all variables was compiled for 70 of the 108 patients. Both univariable and multivariable analyses were performed to determine whether the molecular data singly or in combination offer advantages over tumor type and grade for prediction of overall survival (OS) and/or progression-free rate (PFR).
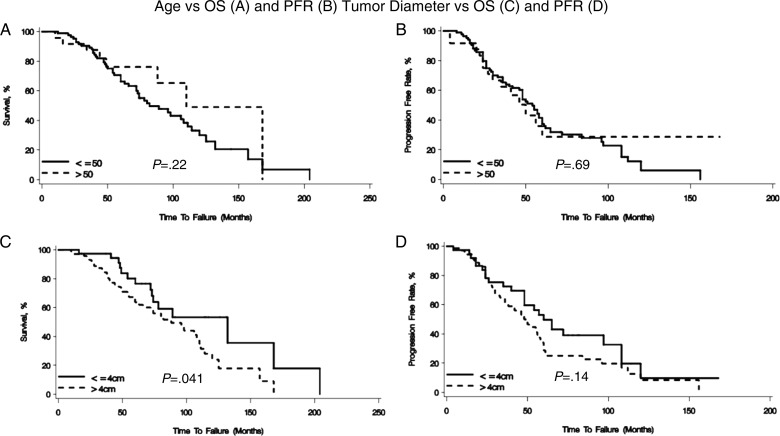
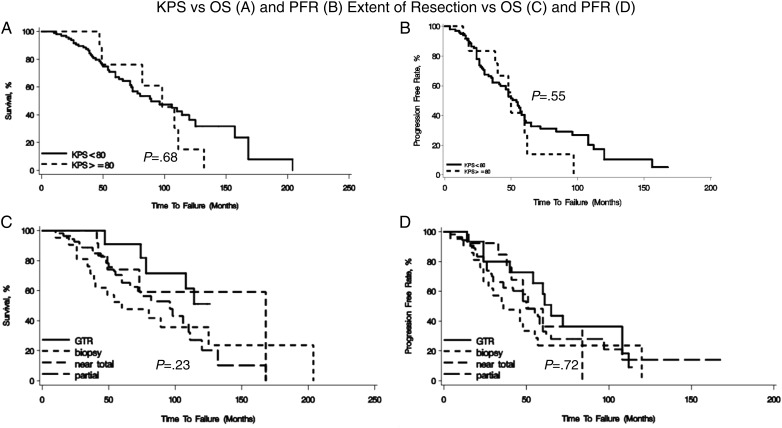
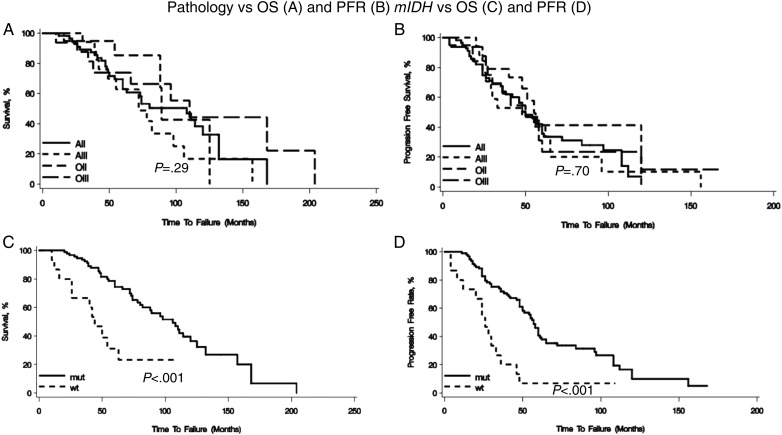
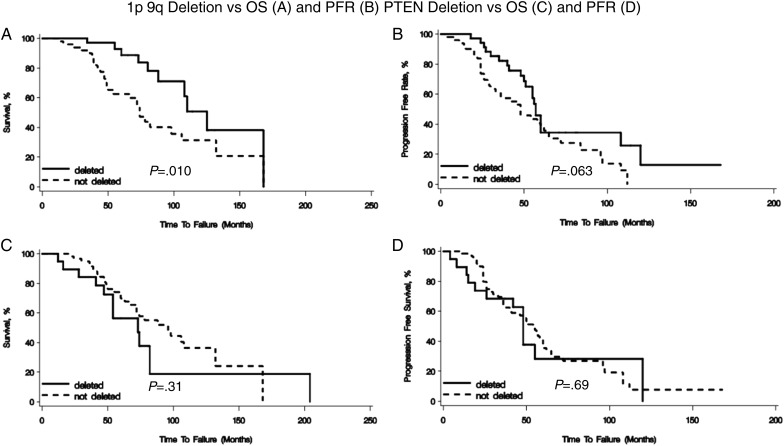
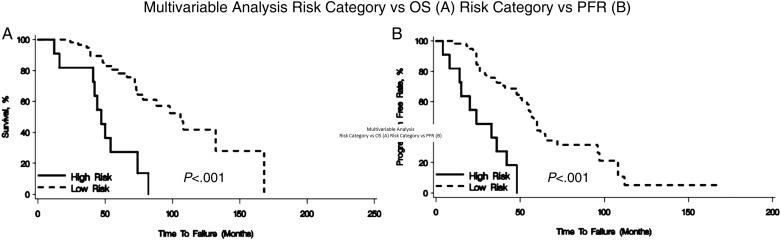
Results: Patient age, clinical variables (tumor diameter, extent of resection, performance status), and pathology (tumor type and grade) were not predictive of OS or PFR. IDH mutation status alone was predictive of longer OS and PFR for the entire group of tumors; 1p/19q deletion alone was predictive of OS but not PFR. In the multivariable analysis, none of the clinical or demographic factors were predictive of OS or PFR. IDH mutation status, 1p/19q codeletion, and PTEN deletion were predictive of OS (P = .003, P = .005, P = .02, respectively). Both mIDH (P < .001) and the interaction term of 1p/19q and PTEN (P < .001) were found to be predictive of PFR.
Conclusions: We conclude that the combination of mIDH, 1p/19q codeletion, and PTEN deletion may be particularly effective in discriminating good prognosis from poor prognosis hemispheric gliomas. We propose that such a scheme merits testing on larger prospective cohorts. Should our findings be confirmed, routine clinical analysis of hemispheric gliomas for mIDH, 1p/19q codeletion, and PTEN deletion would be justified.
Figures
Comment in
-
Editorial commentary on "Analysis of IDH mutation, 1p19q deletion, and PTEN loss delineates prognosis in clinical low-grade gliomas".Neuro Oncol. 2014 Jul;16(7):891-2. doi: 10.1093/neuonc/nou100. Neuro Oncol. 2014. PMID: 24861880 Free PMC article. No abstract available.
References
-
- Chang EF, Clark A, Jensen RL, et al. Multiinstitutional validation of the University of California at San Francisco low-grade glioma prognostic scoring system. J Neurosurg. 2009;111:203–210. - PubMed
-
- Cairncross JG, Ueki K, Zlatescu MC, et al. Specific genetic predictors of chemotherapeutic response and survival in patients with anaplastic oligodendrogliomas. J Natl Cancer Inst. 1998;90:1473–1479. - PubMed
-
- von Deimling A, von Ammon K, Schoenfeld D, et al. Subsets of glioblastoma multiforme defined by molecular genetic analysis. Brain Pathol. 1993;3:19–26. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
