

Integrating diffusion kurtosis imaging, dynamic susceptibility-weighted contrast-enhanced MRI, and short echo time chemical shift imaging for grading gliomas
- PMID: 24470551
- PMCID: PMC4057134
- DOI: 10.1093/neuonc/not304
Integrating diffusion kurtosis imaging, dynamic susceptibility-weighted contrast-enhanced MRI, and short echo time chemical shift imaging for grading gliomas
Abstract
Background: We assessed the diagnostic accuracy of diffusion kurtosis imaging (DKI), dynamic susceptibility-weighted contrast-enhanced (DSC) MRI, and short echo time chemical shift imaging (CSI) for grading gliomas.
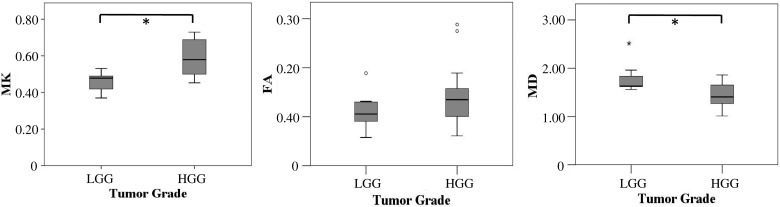
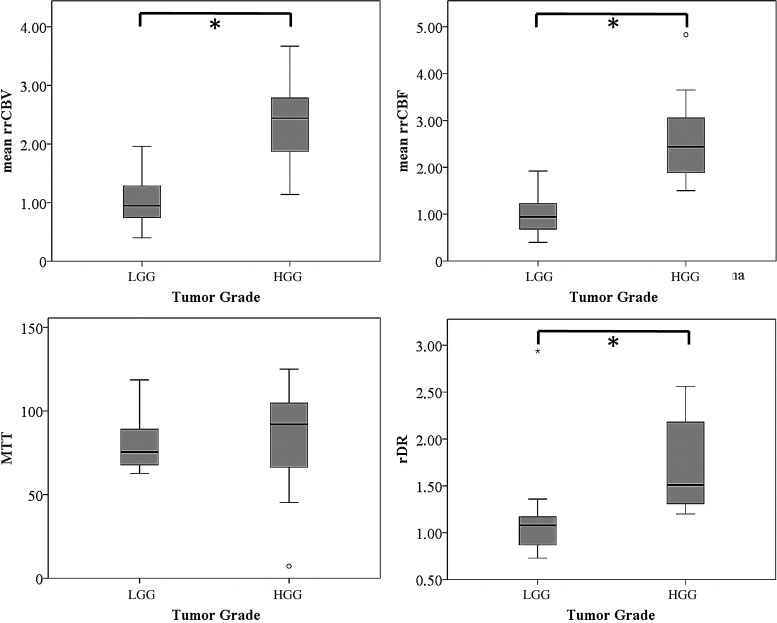
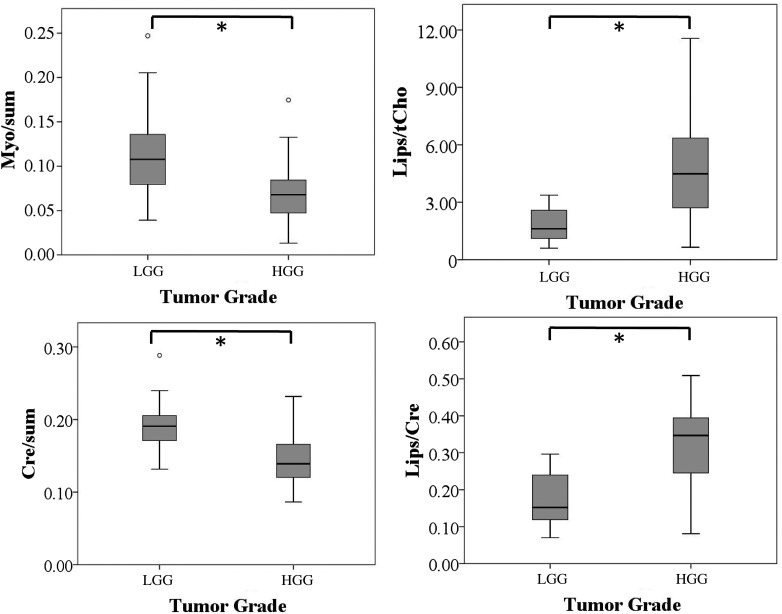
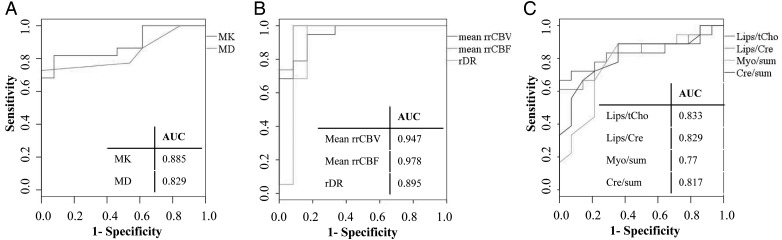
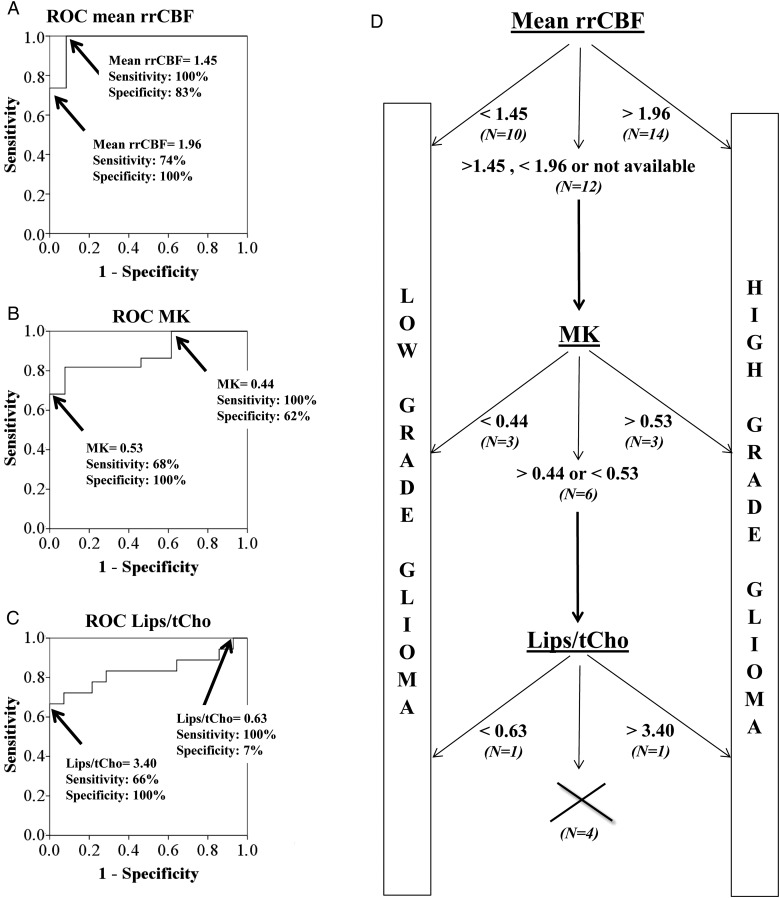
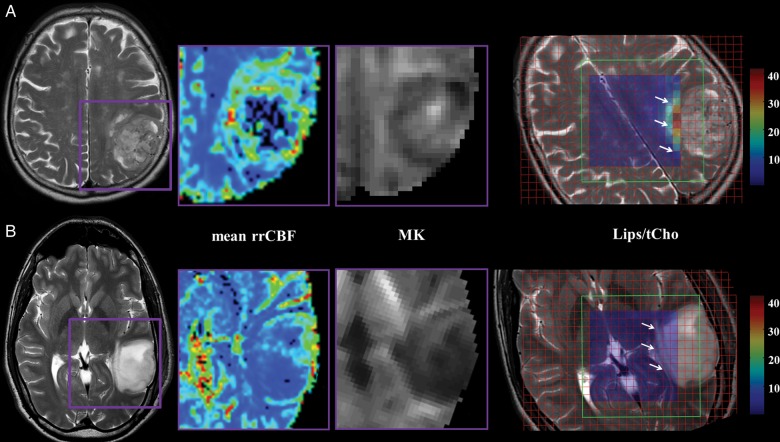
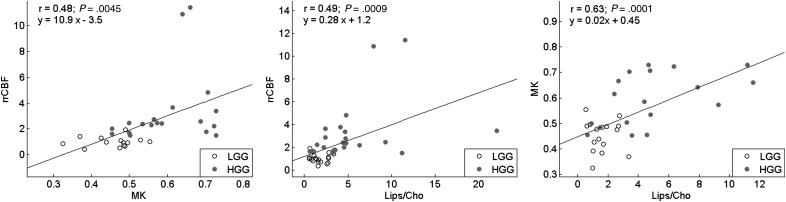
Methods: In this prospective study, 35 patients with cerebral gliomas underwent DKI, DSC, and CSI on a 3 T MR scanner. Diffusion parameters were mean diffusivity (MD), fractional anisotropy, and mean kurtosis (MK). Perfusion parameters were mean relative regional cerebral blood volume (rrCBV), mean relative regional cerebral blood flow (rrCBF), mean transit time, and relative decrease ratio (rDR). The diffusion and perfusion parameters along with 12 CSI metabolite ratios were compared among 22 high-grade gliomas and 14 low-grade gliomas (Mann-Whitney U-test, P < .05). Classification accuracy was determined with a linear discriminant analysis for each MR modality independently. Furthermore, the performance of a multimodal analysis is reported, using a decision-tree rule combining the statistically significant DKI, DSC-MRI, and CSI parameters with the lowest P-value. The proposed classifiers were validated on a set of subsequently acquired data from 19 clinical patients.
Results: Statistically significant differences among tumor grades were shown for MK, MD, mean rrCBV, mean rrCBF, rDR, lipids over total choline, lipids over creatine, sum of myo-inositol, and sum of creatine. DSC-MRI proved to be the modality with the best performance when comparing modalities individually, while the multimodal decision tree proved to be most accurate in predicting tumor grade, with a performance of 86%.
Conclusions: Combining information from DKI, DSC-MRI, and CSI increases diagnostic accuracy to differentiate low- from high-grade gliomas, possibly providing diagnosis for the individual patient.
Figures
References
-
- McGirt MJ, Woodworth GF, Coon AL, et al. Independent predictors of morbidity after image-guided stereotactic brain biopsy: a risk assessment of 270 cases. J Neurosurg. 2005;102(5):897–901. - PubMed
-
- Scott JN, Brasher PM, Sevick RJ, Rewcastle NB, Forsyth PA. How often are nonenhancing supratentorial gliomas malignant? A population study. Neurology. 2002;59(6):947–949. - PubMed
-
- Heiss WD, Raab P, Lanfermann H. Multimodality assessment of brain tumors and tumor recurrence. J Nucl Med. 2011;52(10):1585–1600. - PubMed
-
- Morita N, Harada M, Otsuka H, Melhem ER, Nishitani H. Clinical application of MR spectroscopy and imaging of brain tumor. Magn Reson Med Sci. 2010;9(4):167–175. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
