

Phase I/II study of erlotinib and temsirolimus for patients with recurrent malignant gliomas: North American Brain Tumor Consortium trial 04-02
- PMID: 24470557
- PMCID: PMC3956354
- DOI: 10.1093/neuonc/not247
Phase I/II study of erlotinib and temsirolimus for patients with recurrent malignant gliomas: North American Brain Tumor Consortium trial 04-02
Abstract
Background: Inhibition of epidermal growth factor receptor (EGFR) and the mechanistic target of rapamycin (mTOR) may have synergistic antitumor effects in high-grade glioma patients.
Methods: We conducted a phase I/II study of the EGFR inhibitor erlotinib (150 mg/day) and the mTOR inhibitor temsirolimus. Patients initially received temsirolimus 50 mg weekly, and the dose adjusted based on toxicities. In the phase II component, the primary endpoint was 6-month progression-free survival (PFS6) among glioblastoma patients.
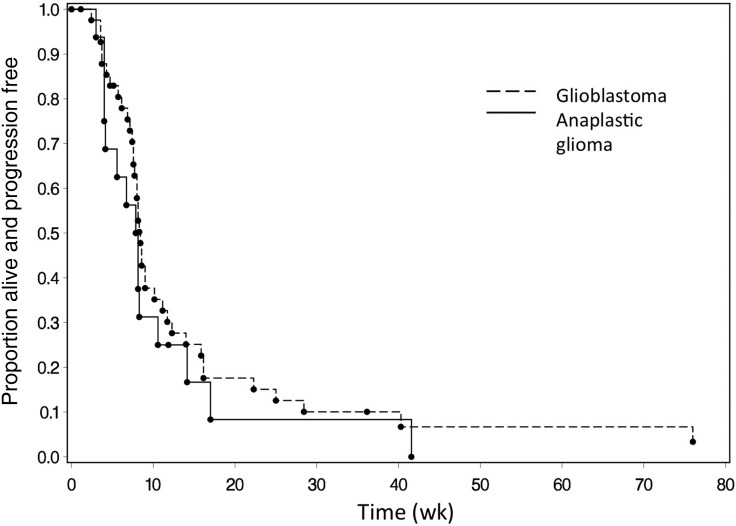
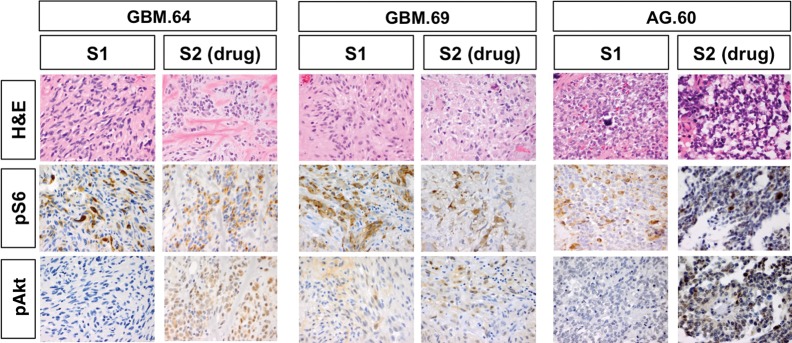
Results: Twenty-two patients enrolled in phase I, 47 in phase II. Twelve phase I patients treated at the maximum tolerated dosage were included in the phase II cohort for analysis. The maximum tolerated dosage was 15 mg temsirolimus weekly with erlotinib 150 mg daily. Dose-limiting toxicities were rash and mucositis. Among 42 evaluable glioblastoma patients, 12 (29%) achieved stable disease, but there were no responses, and PFS6 was 13%. Among 16 anaplastic glioma patients, 1 (6%) achieved complete response, 1 (6%) partial response, and 2 (12.5%) stable disease, with PFS6 of 8%. Tumor levels of both drugs were low, and posttreatment tissue in 3 patients showed no reduction in the mTOR target phosphorylated (phospho-)S6(S235/236) but possible compensatory increase in phospho-Akt(S473). Presence of EGFR variant III, phospho-EGFR, and EGFR amplification did not correlate with survival, but patients with elevated phospho-extracellular signal-regulated kinase or reduced phosphatase and tensin homolog protein expression had decreased progression-free survival at 4 months.
Conclusion: Because of increased toxicity, the maximum tolerated dosage of temsirolimus in combination with erlotinib proved lower than expected. Insufficient tumor drug levels and redundant signaling pathways may partly explain the minimal antitumor activity noted.
Keywords: anaplastic glioma; clinical trial; epidermal growth factor; erlotinib; glioblastoma; temsirolimus.
Figures
References
-
- CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2004–2007. Hinsdale IL: Central Brain Tumor Registry of the United States; 2011.
-
- Wen PY, Kesari S. Malignant gliomas in adults. N Engl J Med. 2008;359:492–507. - PubMed
-
- Wong ET, Hess KR, Gleason MJ, et al. Outcomes and prognostic factors in recurrent glioma patients enrolled onto phase II clinical trials. J Clin Oncol. 1999;17:2572–2578. - PubMed
-
- Nicholas MK, Lukas RV, Jafri NF, et al. Epidermal growth factor receptor–mediated signal transduction in the development and therapy of gliomas. Clin Cancer Res. 2006;12:7261–7270. - PubMed
-
- Frederick L, Wang XY, Eley G, et al. Diversity and frequency of epidermal growth factor receptor mutations in human glioblastomas. Cancer Res. 2000;60:1383–1387. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
