

Envelope analysis of the airflow signal to improve polysomnographic assessment of sleep disordered breathing
- PMID: 24470709
- PMCID: PMC3902884
- DOI: 10.5665/sleep.3338
Envelope analysis of the airflow signal to improve polysomnographic assessment of sleep disordered breathing
Abstract
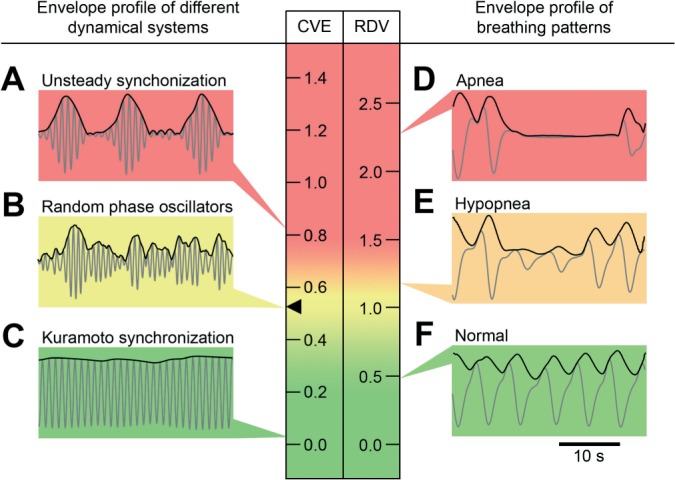
Study objectives: Given the detailed respiratory waveform signal provided by the nasal cannula in polysomnographic (PSG) studies, to quantify sleep breathing disturbances by extracting a continuous variable based on the coefficient of variation of the envelope of that signal.
Design: Application of an algorithm for envelope analysis to standard nasal cannula signal from actual polysomnographic studies.
Setting: PSG recordings from a sleep disorders center were analyzed by an algorithm developed on the Igor scientific data analysis software.
Patients or participants: Recordings representative of different degrees of sleep disordered breathing (SDB) severity or illustrative of the covariation between breathing and particularly relevant factors and variables.
Interventions: The method calculated the coefficient of variation of the envelope for each 30-second epoch. The normalized version of that coefficient was defined as the respiratory disturbance variable (RDV). The method outcome was the all-night set of RDV values represented as a time series.
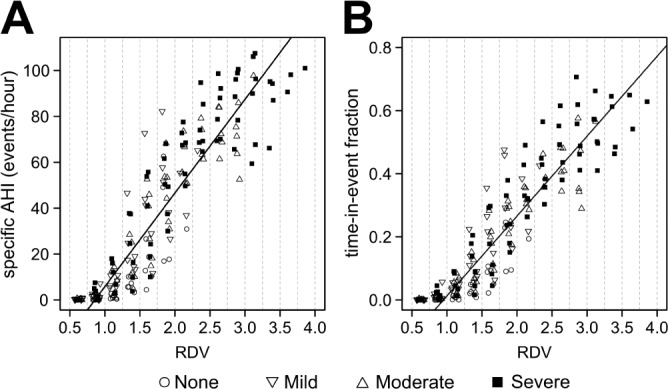
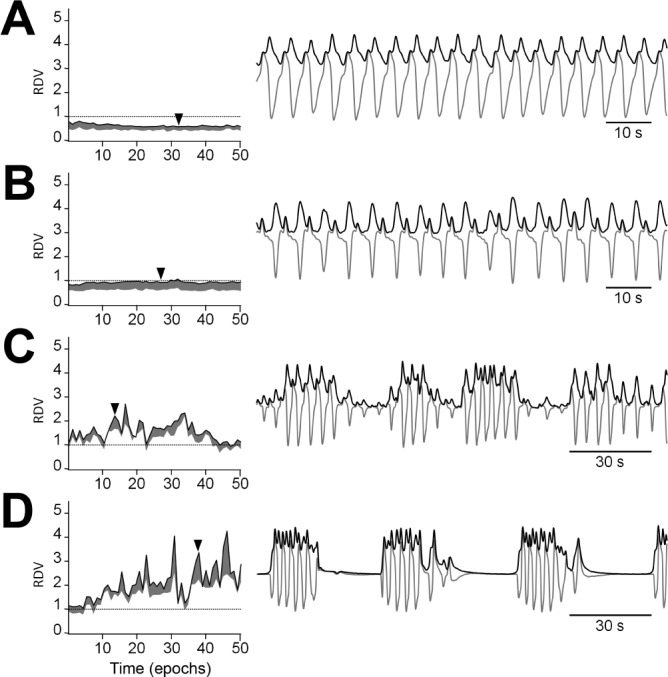
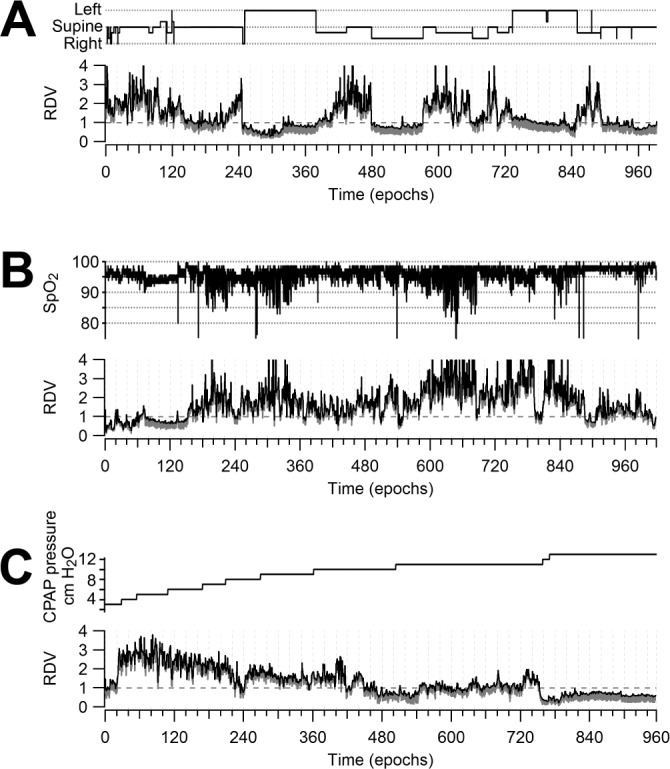
Measurements and results: RDV quantitatively reflected departure from normal sinusoidal breathing at each epoch, providing an intensity scale for disordered breathing. RDV dynamics configured itself in recognizable patterns for the airflow limitation (e.g., in UARS) and the apnea/hypopnea regimes. RDV reliably highlighted clinically meaningful associations with staging, body position, oximetry, or CPAP titration.
Conclusions: Respiratory disturbance variable can assess sleep breathing disturbances as a gradual phenomenon while providing a comprehensible and detailed representation of its dynamics. It may thus improve clinical diagnosis and provide a revealing descriptive tool for mechanistic sleep disordered breathing modeling. Respiratory disturbance variable may contribute to attaining simplified screening methodologies, novel diagnostic criteria, and insightful research tools.
Keywords: Signal envelope analysis; medical informatics applications; nasal cannula / pressure; polysomnography; sleep apnea syndromes; transducer; upper airway resistance sleep apnea syndrome.
Figures



References
-
- Duran J, Esnaola S, Rubio R, Iztueta A. Obstructive sleep apnea-hypopnea and related clinical features in a population-based sample of subjects aged 30 to 70 yr. Am J Respir Crit Care Med. 2001;163(3 Pt 1):685–9. - PubMed
-
- George CF. Sleep apnea, alertness, and motor vehicle crashes. Am J Respir Crit Care Med. 2007;176:954–6. - PubMed
-
- Nieto FJ, Young TB, Lind BK, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. Sleep Heart Health Study. JAMA. 2000;283:1829–36. - PubMed
-
- Peppard PE, Szklo-Coxe M, Hla KM, Young T. Longitudinal association of sleep-related breathing disorder and depression. Arch Intern Med. 2006;166:1709–15. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
