

The severe acute respiratory syndrome epidemic in mainland China dissected
- PMID: 24470901
- PMCID: PMC3892599
- DOI: 10.4081/idr.2011.e2
The severe acute respiratory syndrome epidemic in mainland China dissected
Abstract
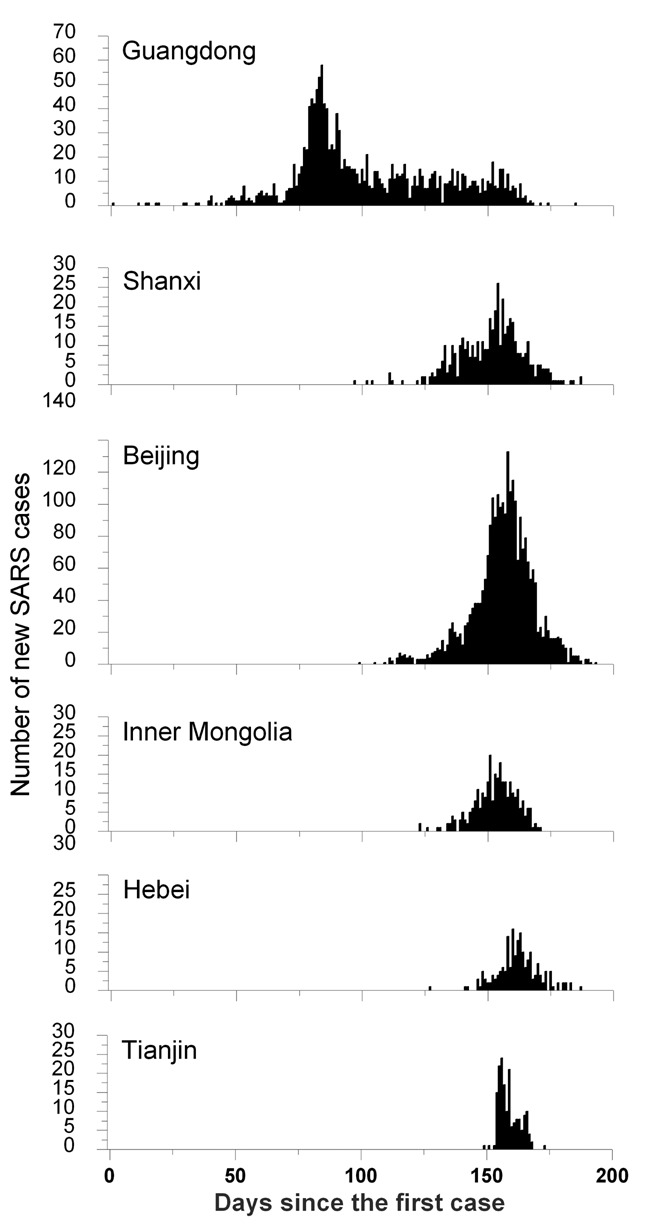
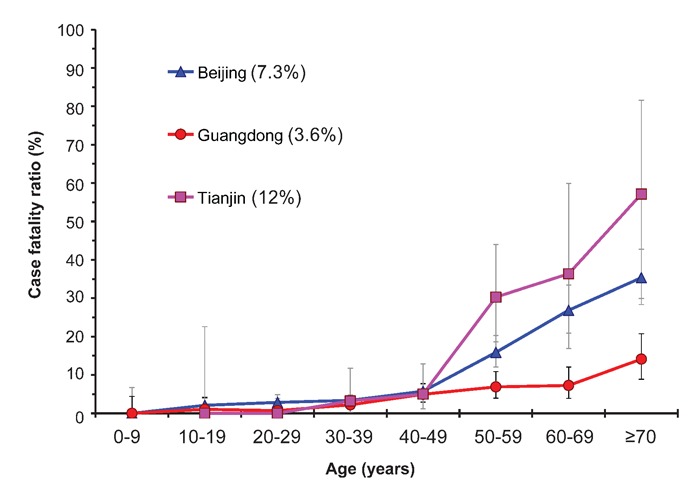
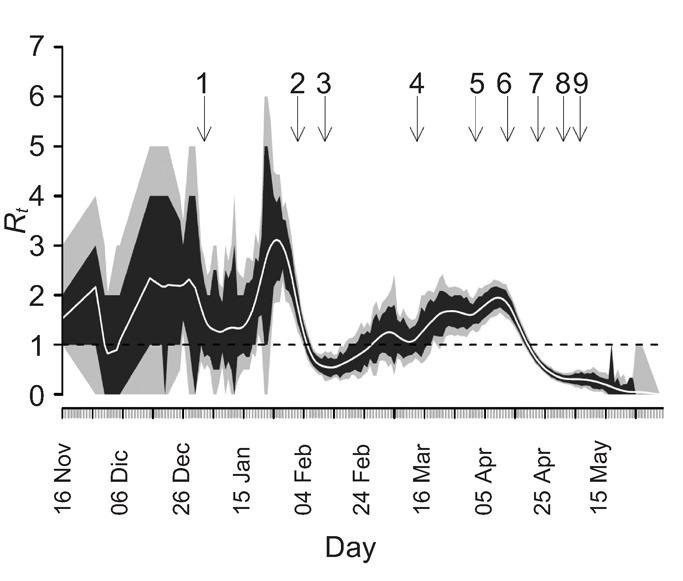
This paper provides a review of a recently published series of studies that give a detailed and comprehensive documentation of the severe acute respiratory syndrome (SARS) epidemic in mainland China, which severely struck the country in the spring of 2003. The epidemic spanned a large geographical extent but clustered in two areas: first in Guangdong Province, and about 3 months later in Beijing with its surrounding areas. Reanalysis of all available epidemiological data resulted in a total of 5327 probable cases of SARS, of whom 343 died. The resulting case fatality ratio (CFR) of 6.4% was less than half of that in other SARS-affected countries or areas, and this difference could only partly be explained by younger age of patients and higher number of community acquired infections. Analysis of the impact of interventions demonstrated that strong political commitment and a centrally coordinated response was the most important factor to control SARS in mainland China, whereas the most stringent control measures were all initiated when the epidemic was already dying down. The long-term economic consequence of the epidemic was limited, much consumption was merely postponed, but for Beijing irrecoverable losses to the tourist sector were considerable. An important finding from a cohort study was that many former SARS patients currently suffer from avascular osteonecrosis, as a consequence of the treatment with corticosteroids during their infection. The SARS epidemic provided valuable information and lessons relevant in controlling outbreaks of newly emerging infectious diseases, and has led to fundamental reforms of the Chinese health system. In particular, a comprehensive nationwide internet-based disease reporting system was established.
Keywords: China; avascular necrosis; case fatality ratio; epidemic preparedness.; severe acute respiratory syndrome.
Conflict of interest statement
Conflict of interest: the authors report no conflicts of interest.
Figures
Similar articles
-
What we have learnt from the SARS epdemics in mainland China?Glob Health J. 2019 Sep;3(3):55-59. doi: 10.1016/j.glohj.2019.09.003. Epub 2019 Sep 28. Glob Health J. 2019. Retraction in: Glob Health J. 2021 Mar;5(1):e1. doi: 10.1016/j.glohj.2020.12.002. PMID: 32501415 Free PMC article. Retracted.
-
Case fatality of SARS in mainland China and associated risk factors.Trop Med Int Health. 2009 Nov;14 Suppl 1(Suppl 1):21-7. doi: 10.1111/j.1365-3156.2008.02147.x. Epub 2009 Apr 17. Trop Med Int Health. 2009. PMID: 19508439 Free PMC article.
-
Geographical spread of SARS in mainland China.Trop Med Int Health. 2009 Nov;14 Suppl 1(Suppl 1):14-20. doi: 10.1111/j.1365-3156.2008.02189.x. Epub 2009 Jun 5. Trop Med Int Health. 2009. PMID: 19508436 Free PMC article.
-
No evidence of over-reporting of SARS in mainland China.Trop Med Int Health. 2009 Nov;14 Suppl 1:46-51. doi: 10.1111/j.1365-3156.2009.02300.x. Trop Med Int Health. 2009. PMID: 19814761 Review.
-
Anatomy of the epidemiological literature on the 2003 SARS outbreaks in Hong Kong and Toronto: a time-stratified review.PLoS Med. 2010 May 4;7(5):e1000272. doi: 10.1371/journal.pmed.1000272. PLoS Med. 2010. PMID: 20454570 Free PMC article. Review.
Cited by
-
Assessment of transmissibility and measures effectiveness of SARS in 8 regions, China, 2002-2003.Front Cell Infect Microbiol. 2023 Aug 10;13:1212473. doi: 10.3389/fcimb.2023.1212473. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 37637464 Free PMC article.
-
A Single-Cell RNA Expression Map of Human Coronavirus Entry Factors.SSRN [Preprint]. 2020 May 27:3611279. doi: 10.2139/ssrn.3611279. SSRN. 2020. Update in: Cell Rep. 2020 Sep 22;32(12):108175. doi: 10.1016/j.celrep.2020.108175. PMID: 32714119 Free PMC article. Updated. Preprint.
-
Systematic analysis of infectious disease outcomes by age shows lowest severity in school-age children.Sci Data. 2020 Oct 15;7(1):329. doi: 10.1038/s41597-020-00668-y. Sci Data. 2020. PMID: 33057040 Free PMC article.
-
Advances in the relationship between coronavirus infection and cardiovascular diseases.Biomed Pharmacother. 2020 Jul;127:110230. doi: 10.1016/j.biopha.2020.110230. Epub 2020 May 13. Biomed Pharmacother. 2020. PMID: 32428835 Free PMC article. Review.
-
The Causal Relationship between Eating Animals and Viral Epidemics.Microb Physiol. 2020;30(1-6):2-8. doi: 10.1159/000511192. Epub 2020 Sep 21. Microb Physiol. 2020. PMID: 32957108 Free PMC article. Review.
References
-
- Drosten C, Gunther S, Preiser W, et al. Identification of a novel coronavirus in patients with severe acute respiratory syndrome. N Engl J Med. 2003;348:1967–76. - PubMed
-
- Ksiazek TG, Erdman D, Goldsmith CS, et al. A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med. 2003;348:1953–66. - PubMed
-
- WHO. Severe Acute Respiratory Syndrome (SARS) [cited 2009 12 June 2009];2004 Available from: http://www.who.int/csr/sars/en/
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
