

Comparison of viral load in individuals with and without asthma during infections with rhinovirus
- PMID: 24471509
- PMCID: PMC3977713
- DOI: 10.1164/rccm.201310-1767OC
Comparison of viral load in individuals with and without asthma during infections with rhinovirus
Abstract
Rationale: Most virus-induced attacks of asthma are caused by rhinoviruses (RVs).
Objectives: To determine whether people with asthma are susceptible to an increased viral load during RV infection.
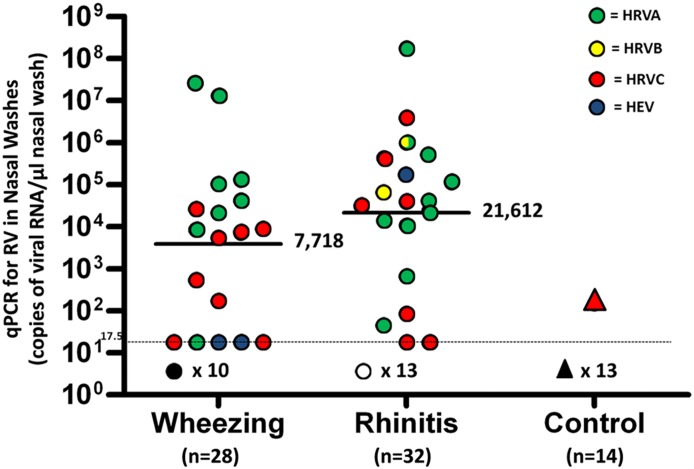
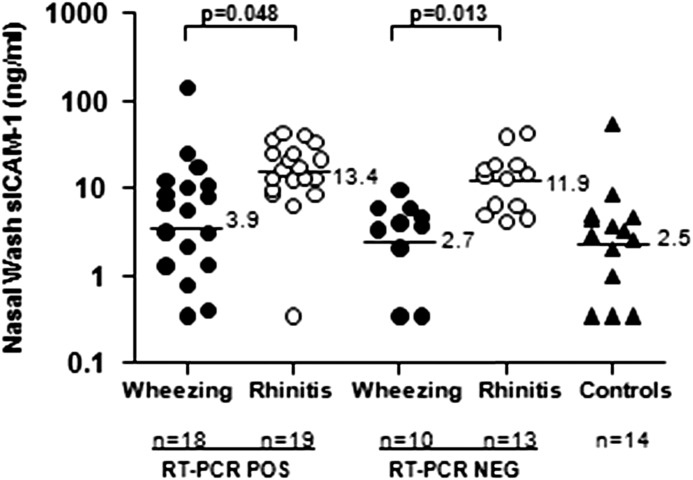
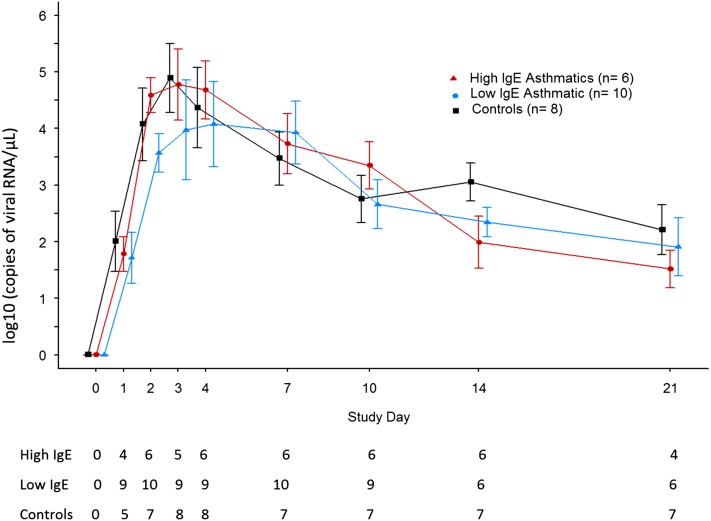
Methods: Seventy-four children (4-18 yr old) were enrolled; 28 with wheezing, 32 with acute rhinitis, and 14 without respiratory tract symptoms. Nasal washes were evaluated using quantitative polymerase chain reaction for RV to judge viral load along with gene sequencing to identify strains of RV. Soluble intercellular adhesion molecule-1, IFN-λ1, and eosinophil cationic protein in nasal washes, along with blood eosinophil counts and total and allergen-specific IgE in sera, were also evaluated. Similar assessments were done in 24 young adults (16 with asthma, 8 without) who participated in an experimental challenge with RV (serotype 16).
Measurements and main results: Fifty-seven percent of wheezing children and 56% with acute rhinitis had nasal washes testing positive for RV. The geometric mean of viral loads by quantitative polymerase chain reaction in washes from wheezing children was 2.8-fold lower, but did not differ significantly from children with rhinitis (7,718 and 21,612 copies of viral RNA per microliter nasal wash, respectively; P = 0.48). The odds for wheezing were increased if children who tested positive for RV were sensitized to one or more allergens (odds ratio, 3.9; P = 0.02). Similarly, neither peak nor cumulative viral loads differed significantly in washes from adults with asthma compared with those without asthma during the experimental RV challenge.
Conclusions: During acute symptoms, children infected with RV enrolled for wheezing or acute rhinitis had similar viral loads in their nasal washes, as did adults with and without asthma infected with RV-16 experimentally.
Figures
References
-
- Rakes GP, Arruda E, Ingram JM, Hoover GE, Zambrano JC, Hayden FG, Platts-Mills TAE, Heymann PW. Rhinovirus and respiratory syncytial virus in wheezing children requiring emergency care: IgE and eosinophil analyses. Am J Respir Crit Care Med. 1999;159:785–790. - PubMed
-
- Iwane MK, Prill MM, Lu X, Miller EK, Edwards KM, Hall CB, Griffin MR, Staat MA, Anderson LJ, Williams JV, et al. Human rhinovirus species associated with hospitalizations for acute respiratory illness in young US children. J Infect Dis. 2011;204:1702–1710. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
