

Nonalcoholic fatty liver disease, liver fibrosis, and cardiometabolic risk factors in adolescence: a cross-sectional study of 1874 general population adolescents
- PMID: 24471572
- PMCID: PMC3955251
- DOI: 10.1210/jc.2013-3612
Nonalcoholic fatty liver disease, liver fibrosis, and cardiometabolic risk factors in adolescence: a cross-sectional study of 1874 general population adolescents
Abstract
Context: The impact of adolescent nonalcoholic fatty liver disease (NAFLD) on health, independent of fat mass, is unclear.
Objective: The objective of the study was to determine the independent (of total body fat) association of ultrasound scan (USS)-determined NAFLD with liver fibrosis, insulin resistance, and dyslipidemia among healthy adolescents.
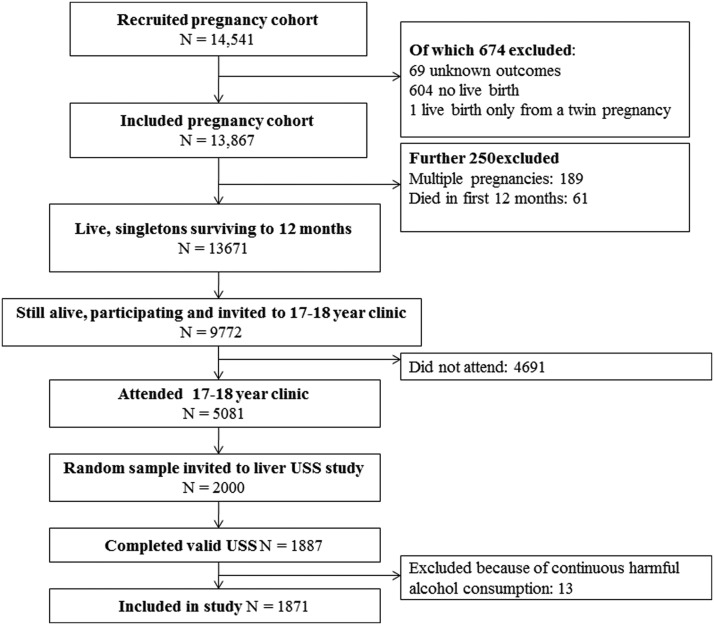
Design: This was a cross-sectional analysis in participants from a UK birth cohort.
Participants: One thousand eight hundred seventy-four (1059 female) individuals of a mean age of 17.9 years participated in the study.
Main outcomes: USS assessed liver stiffness (shear velocity, an indicator of fibrosis) and volume, fasting glucose, insulin, triglycerides, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, alanine amino transferase, aspartate amino transferase, γ-glutamyltransferase, and haptoglobin.
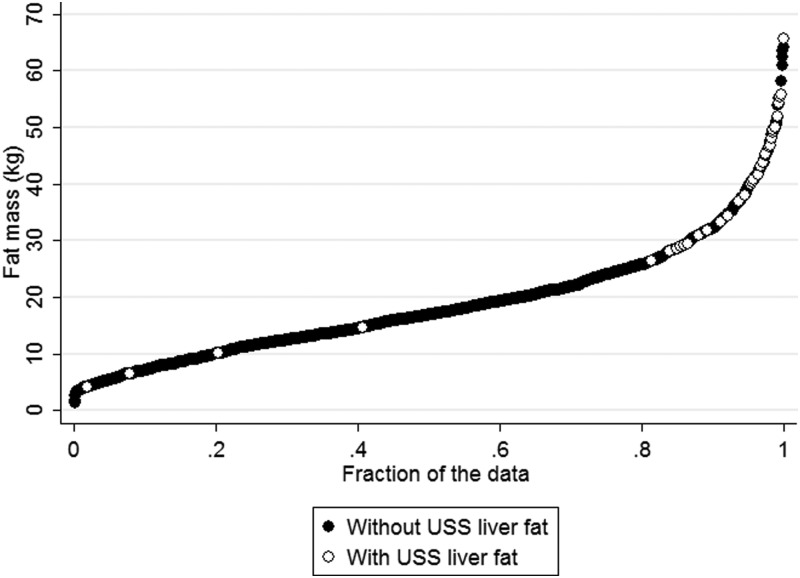
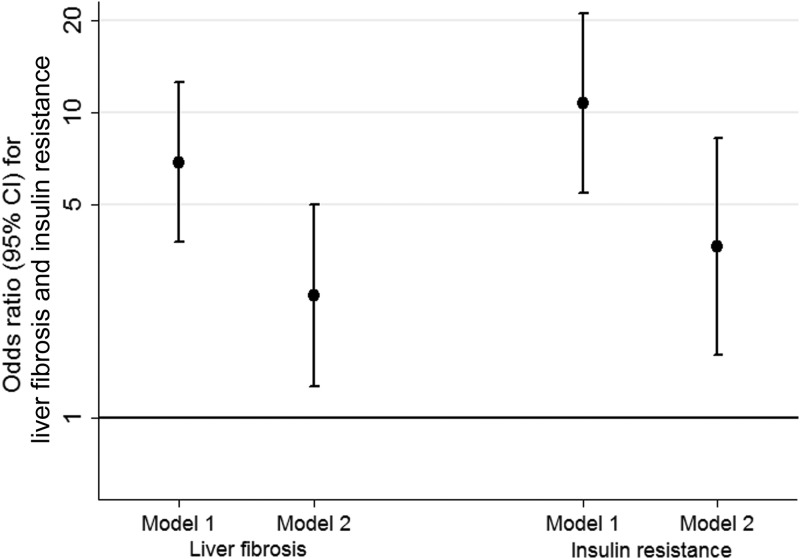
Results: The prevalence of NAFLD was 2.5% [95% confidence interval (CI) 1.8-3.3] and was the same in females and males. Dual-energy X-ray absorptiometry determined total body fat mass was strongly associated with USS NAFLD: odds ratio 3.15 (95% CI 2.44-4.07) per 1 SD (∼10 kg) fat mass. Those with NAFLD had larger liver volumes and greater shear velocity. They also had higher fasting glucose, insulin, triglycerides, low-density lipoprotein cholesterol, alanine amino transferase, aspartate amino transferase, γ-glutamyltransferase, and haptoglobin and lower high-density lipoprotein cholesterol. Most associations were independent of total body fat. For example, after adjustment for fat mass and other confounders, hepatic shear velocity [mean difference 22.8% (95% CI 15.6-30.5)], triglyceride levels [23.6% (95% CI 6.0-44.2)], and insulin [39.4% (95% CI 10.7-75.5)] were greater in those with NAFLD compared with those without NAFLD.
Conclusion: In healthy European adolescents, 2.5% have USS-defined NAFLD. Even after accounting for total body fat, those with NAFLD have more adverse levels of liver fibrosis and cardiometabolic risk factors.
Figures
Comment in
-
Population-based screening programs for nonalcoholic fatty liver disease in youth and clues to prevention.J Clin Endocrinol Metab. 2014 Mar;99(3):774-6. doi: 10.1210/jc.2014-1290. J Clin Endocrinol Metab. 2014. PMID: 24823704 No abstract available.
References
-
- Cheung CR, Kelly DA. Non-alcoholic fatty liver disease in children. BMJ. 2011;343:d4460. - PubMed
-
- Alisi A, Feldstein AE, Villani A, Raponi M, Nobili V. Pediatric nonalcoholic fatty liver disease: a multidisciplinary approach. Nat Rev Gastroenterol Hepatol. 2012;9:152–161 - PubMed
-
- Vajro P, Lenta S, Socha P, et al. Diagnosis of nonalcoholic fatty liver disease in children and adolescents: position paper of the ESPGHAN Hepatology Committee. J Pediatr Gastroenterol Nutr. 2012;54:700–713 - PubMed
-
- Della CC, Alisi A, Saccari A, De Vito R, Vania A, Nobili V. Nonalcoholic fatty liver in children and adolescents: an overview. J Adolesc Health. 2012;51:305–312 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
