

Prognostic significance of adenocarcinoma in situ, minimally invasive adenocarcinoma, and nonmucinous lepidic predominant invasive adenocarcinoma of the lung in patients with stage I disease
- PMID: 24472852
- PMCID: PMC4164170
- DOI: 10.1097/PAS.0000000000000134
Prognostic significance of adenocarcinoma in situ, minimally invasive adenocarcinoma, and nonmucinous lepidic predominant invasive adenocarcinoma of the lung in patients with stage I disease
Abstract
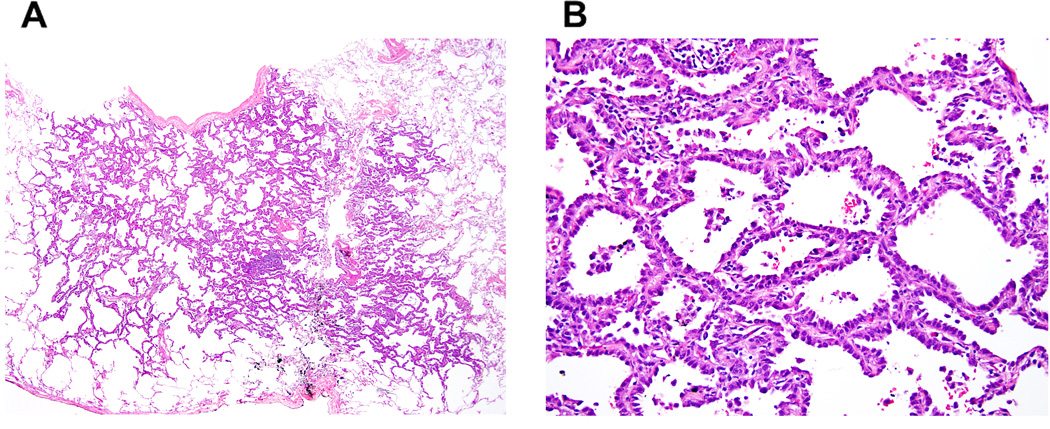
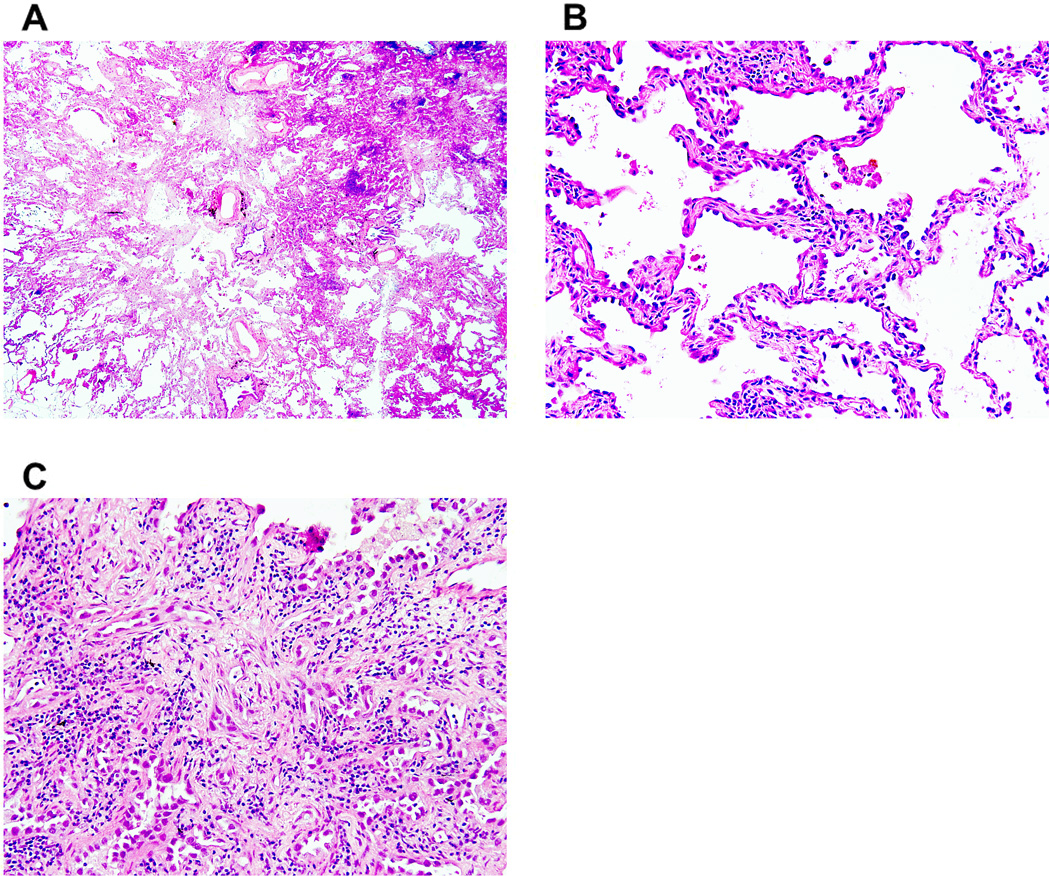
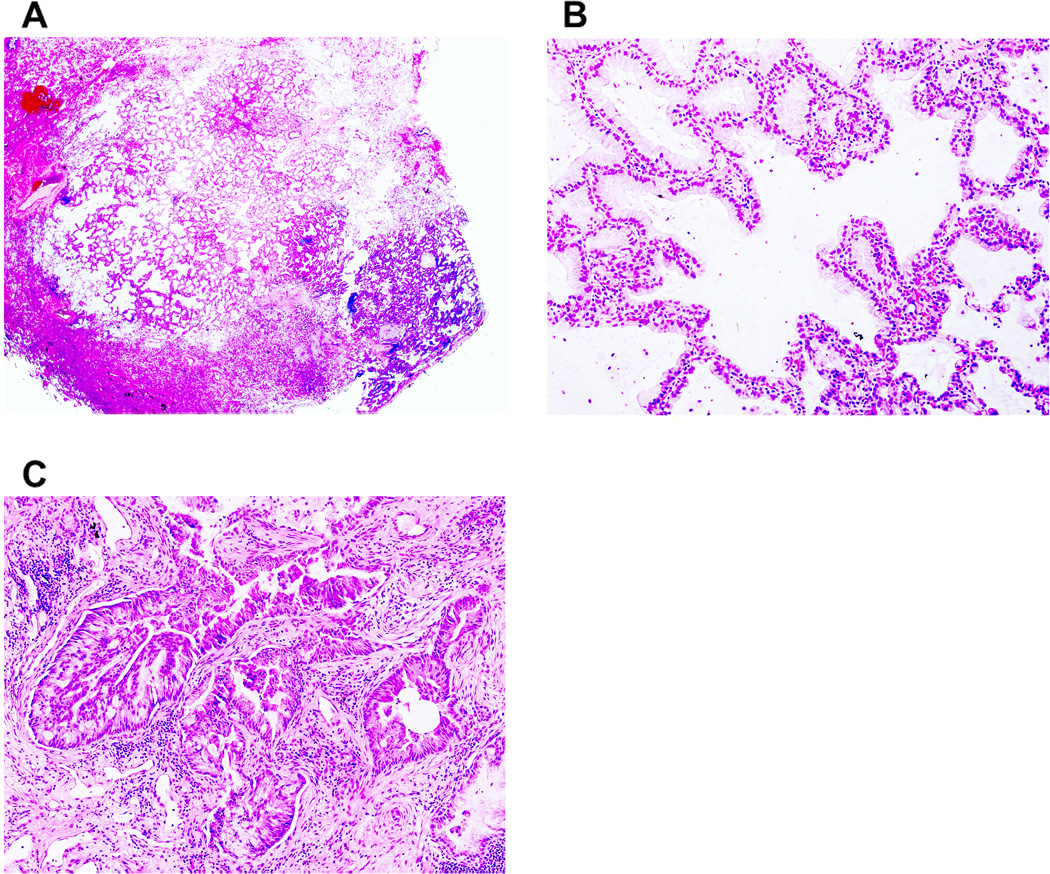
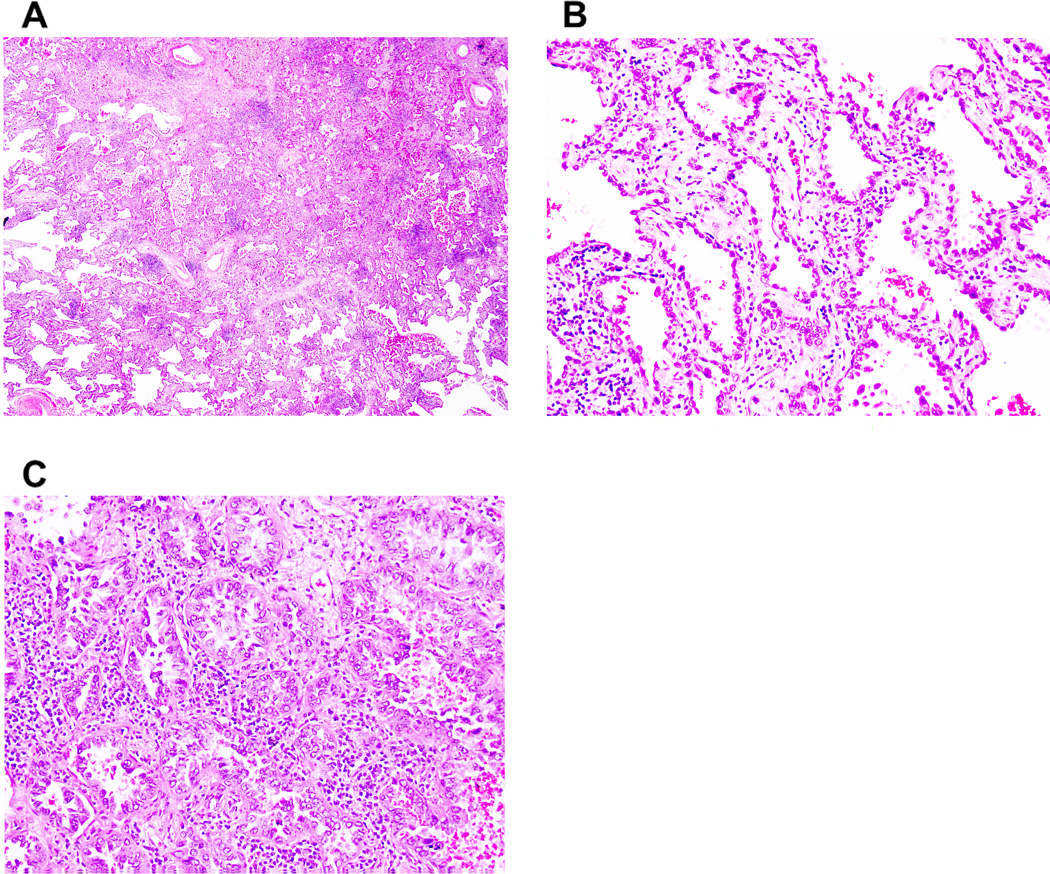
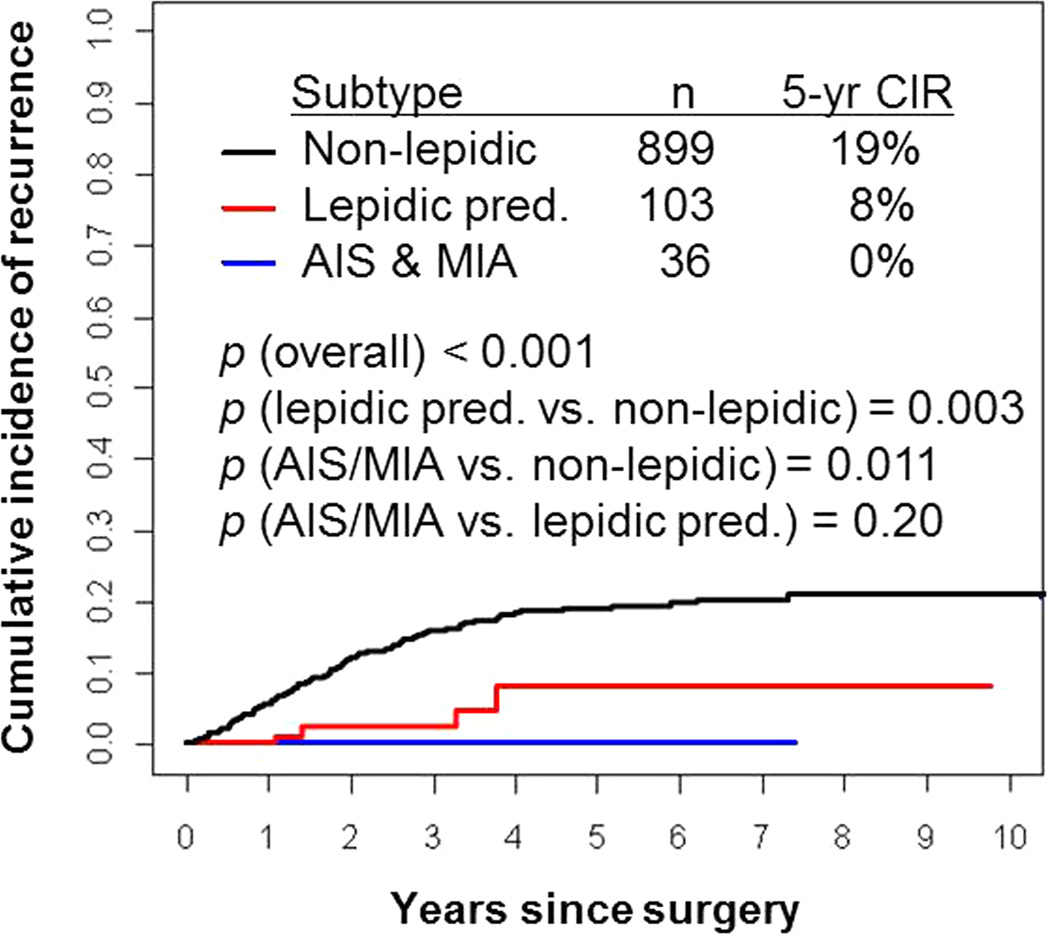
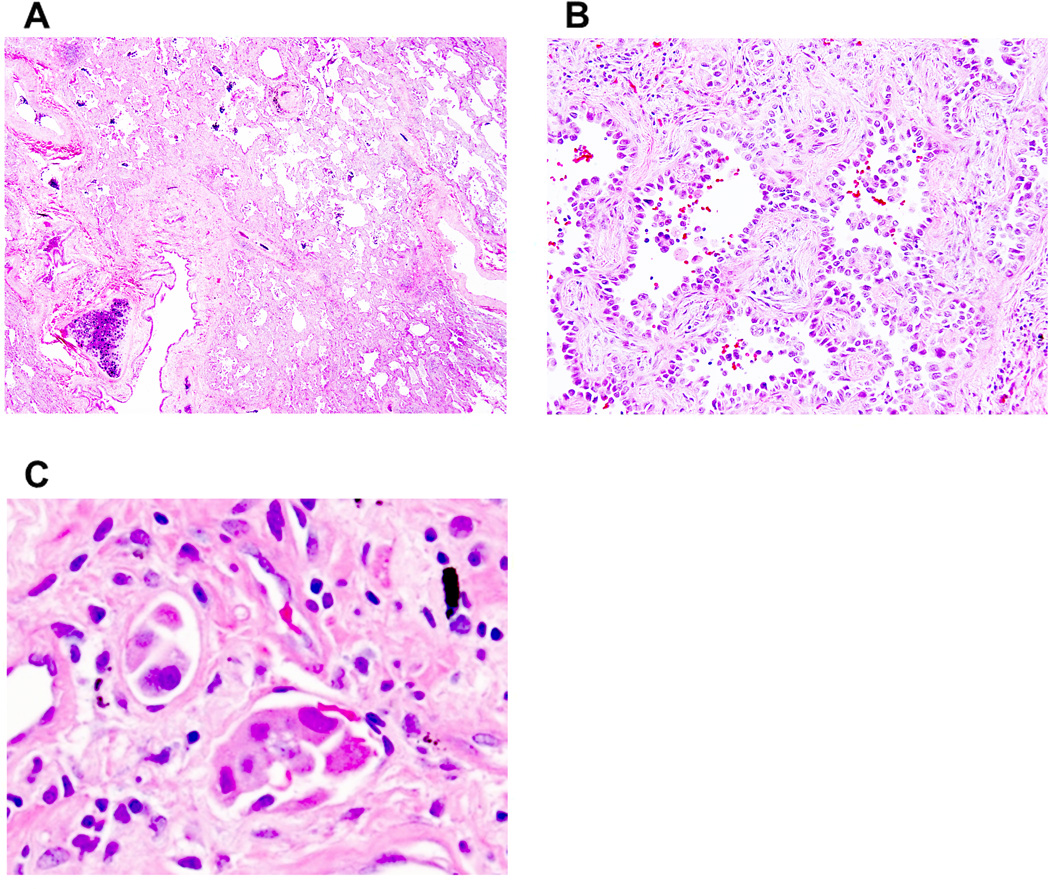
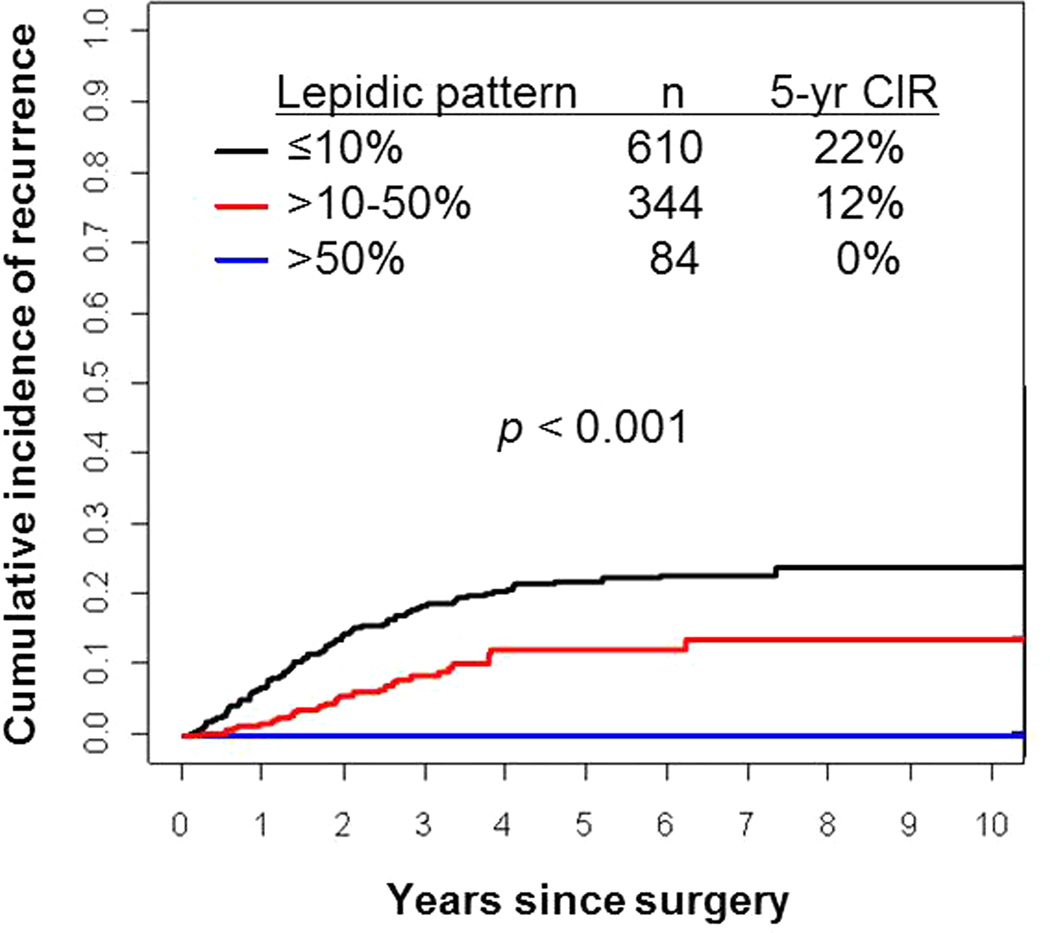
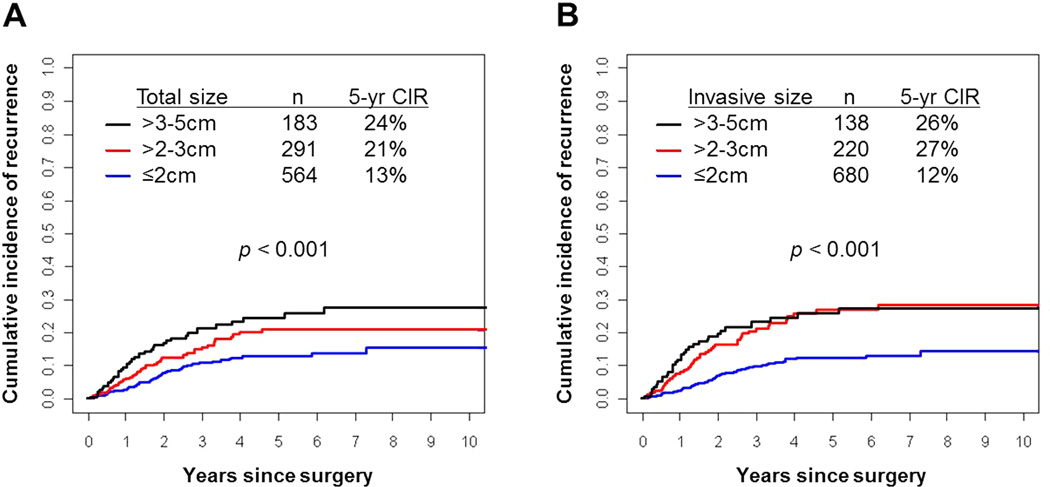
According to the IASLC/ATS/ERS classification, the lepidic predominant pattern consists of 3 subtypes: adenocarcinoma in situ (AIS), minimally invasive adenocarcinoma (MIA), and nonmucinous lepidic predominant invasive adenocarcinoma. We reviewed tumor slides from 1038 patients with stage I lung adenocarcinoma, recording the percentage of each histologic pattern and measuring the invasive tumor size. Tumors were classified according to the IASLC/ATS/ERS classification: 2 were AIS, 34 MIA, and 103 lepidic predominant invasive. Cumulative incidence of recurrence (CIR) was used to estimate the probability of recurrence. Patients with AIS and MIA experienced no recurrences. Patients with lepidic predominant invasive tumors had a lower risk for recurrence (5-y CIR, 8%) than nonlepidic predominant tumors (n=899; 19%; P=0.003). Patients with >50% lepidic pattern tumors experienced no recurrences (n=84), those with >10% to 50% lepidic pattern tumors had an intermediate risk for recurrence (n=344; 5-y CIR, 12%), and those with ≤10% lepidic pattern tumors had the highest risk (n=610; 22%; P<0.001). CIR was lower for patients with ≤2 cm tumors than for those with >2 to 3 cm tumors (for both total and invasive tumor size), with the difference more pronounced for invasive tumor size (5-y CIR, 13% vs. 21% [total size; P=0.022] and 12% vs. 27% [invasive size; P<0.001]). Most patients with lepidic predominant adenocarcinoma who experienced a recurrence had potential risk factors, including sublobar resection with close margins (≤0.5 cm; n=2), 20% to 30% micropapillary component (n=2), and lymphatic or vascular invasion (n=2). It therefore may be possible to identify lepidic predominant adenocarcinomas that carry a low or high risk for recurrence.
Conflict of interest statement
All authors affirm no actual or potential conflicts of interest, including any financial, personal, or other relationships with other people or organizations.
Figures
References
-
- Travis W, Brambilla E, Muller-Hermelink H, Harris C World Health Organization Classification of Tumours. Tumours of the Lung, Pleura, Thymus, and Heart. IARC Press; Lyon, France: 2004. Pathology and Genetics.
-
- Jones KD. Whence Lepidic? Arch Pathol Lab Med. 2013 Aug 12; [Epub ahead of print]. - PubMed
-
- Noguchi M, Morikawa A, Kawasaki M, et al. Small adenocarcinoma of the lung. Histologic characteristics and prognosis. Cancer. 1995;75(12):2844–2852. - PubMed
-
- Sakurai H, Maeshima A, Watanabe S, et al. Grade of stromal invasion in small adenocarcinoma of the lung: histopathological minimal invasion and prognosis. Am J Surg Pathol. 2004;28(2):198–206. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
