

Association between body mass index and cardiovascular disease mortality in east Asians and south Asians: pooled analysis of prospective data from the Asia Cohort Consortium
- PMID: 24473060
- PMCID: PMC3788174
- DOI: 10.1136/bmj.f5446
Association between body mass index and cardiovascular disease mortality in east Asians and south Asians: pooled analysis of prospective data from the Asia Cohort Consortium
Abstract
Objective: To evaluate the association between body mass index and mortality from overall cardiovascular disease and specific subtypes of cardiovascular disease in east and south Asians.
Design: Pooled analyses of 20 prospective cohorts in Asia, including data from 835,082 east Asians and 289,815 south Asians. Cohorts were identified through a systematic search of the literature in early 2008, followed by a survey that was sent to each cohort to assess data availability.
Setting: General populations in east Asia (China, Taiwan, Singapore, Japan, and Korea) and south Asia (India and Bangladesh).
Participants: 1,124,897 men and women (mean age 53.4 years at baseline).
Main outcome measures: Risk of death from overall cardiovascular disease, coronary heart disease, stroke, and (in east Asians only) stroke subtypes.
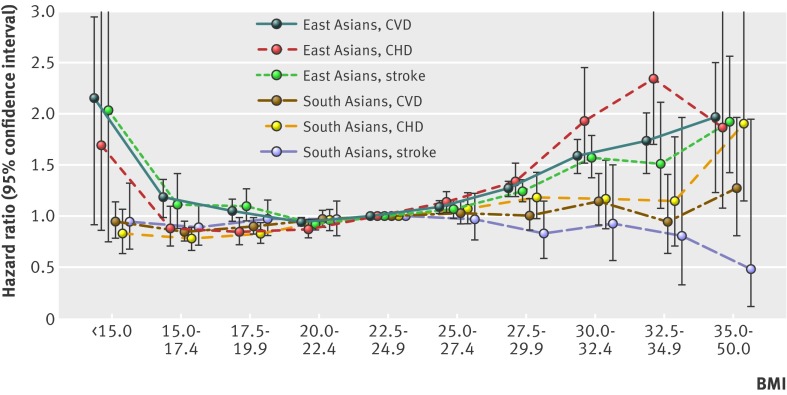
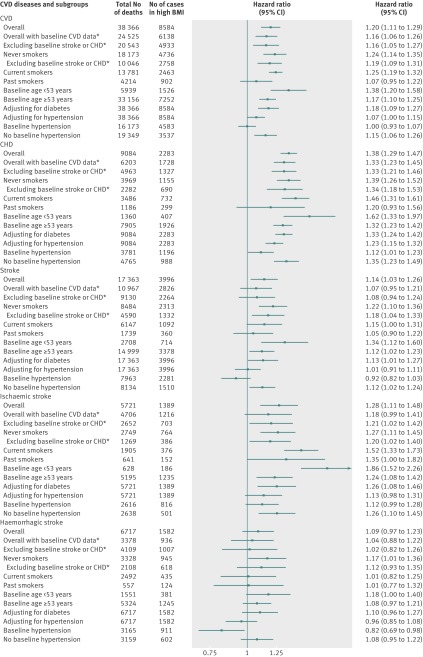
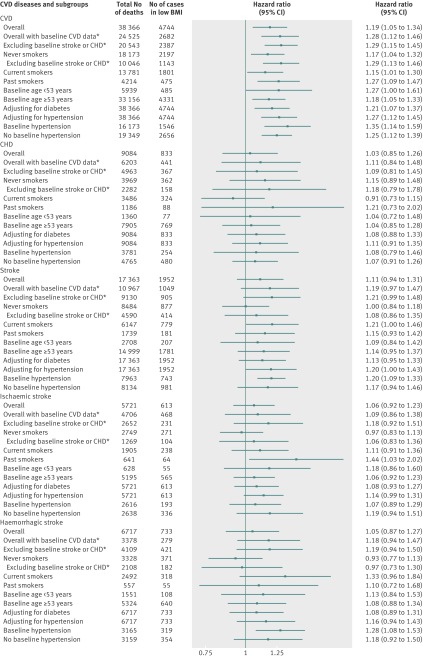
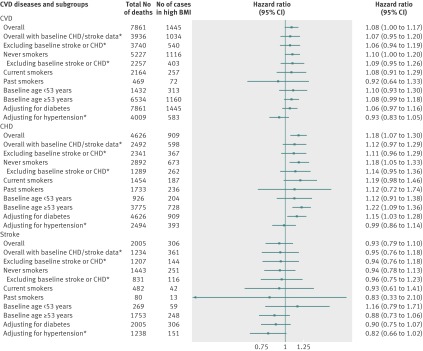
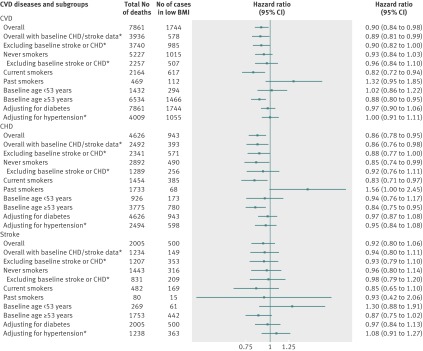
Results: 49,184 cardiovascular deaths (40,791 in east Asians and 8393 in south Asians) were identified during a mean follow-up of 9.7 years. East Asians with a body mass index of 25 or above had a raised risk of death from overall cardiovascular disease, compared with the reference range of body mass index (values 22.5-24.9; hazard ratio 1.09 (95% confidence interval 1.03 to 1.15), 1.27 (1.20 to 1.35), 1.59 (1.43 to 1.76), 1.74 (1.47 to 2.06), and 1.97 (1.44 to 2.71) for body mass index ranges 25.0-27.4, 27.5-29.9, 30.0-32.4, 32.5-34.9, and 35.0-50.0, respectively). This association was similar for risk of death from coronary heart disease and ischaemic stroke; for haemorrhagic stroke, the risk of death was higher at body mass index values of 27.5 and above. Elevated risk of death from cardiovascular disease was also observed at lower categories of body mass index (hazard ratio 1.19 (95% confidence interval 1.02 to 1.39) and 2.16 (1.37 to 3.40) for body mass index ranges 15.0-17.4 and <15.0, respectively), compared with the reference range. In south Asians, the association between body mass index and mortality from cardiovascular disease was less pronounced than that in east Asians. South Asians had an increased risk of death observed for coronary heart disease only in individuals with a body mass index greater than 35 (hazard ratio 1.90, 95% confidence interval 1.15 to 3.12).
Conclusions: Body mass index shows a U shaped association with death from overall cardiovascular disease among east Asians: increased risk of death from cardiovascular disease is observed at lower and higher ranges of body mass index. A high body mass index is a risk factor for mortality from overall cardiovascular disease and for specific diseases, including coronary heart disease, ischaemic stroke, and haemorrhagic stroke in east Asians. Higher body mass index is a weak risk factor for mortality from cardiovascular disease in south Asians.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- World Health Organization. The atlas of heart disease and stroke. WHO, 2004.
-
- Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular diseases: part I: general considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation 2001;104:2746-53. - PubMed
-
- Murray CJL, Lopez AD, eds. The global burden of disease: a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. Harvard School of Public Health, 1996.
-
- Zhang XH, Guan T, Mao J, Liu L. Disparity and its time trends in stroke mortality between urban and rural populations in China 1987 to 2001: changing patterns and their implications for public health policy. Stroke 2007;38:3139-44. - PubMed
Publication types
MeSH terms
Grants and funding
- K01 TW009218/TW/FIC NIH HHS/United States
- P30 CA016672/CA/NCI NIH HHS/United States
- U01 HL072507/HL/NHLBI NIH HHS/United States
- R01CA144034/CA/NCI NIH HHS/United States
- R01CA102484/CA/NCI NIH HHS/United States
- R35CA53890/CA/NCI NIH HHS/United States
- R01CA55069/CA/NCI NIH HHS/United States
- R01CA0403092/CA/NCI NIH HHS/United States
- R37CA70867/CA/NCI NIH HHS/United States
- CRUK_/Cancer Research UK/United Kingdom
- UM1 CA173640/CA/NCI NIH HHS/United States
- R01 CA 82729/CA/NCI NIH HHS/United States
- R01CA107431/CA/NCI NIH HHS/United States
- R01CA80205/CA/NCI NIH HHS/United States
- P42ES010349/ES/NIEHS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical