

Comparative effectiveness of exercise and drug interventions on mortality outcomes: metaepidemiological study
- PMID: 24473061
- PMCID: PMC3788175
- DOI: 10.1136/bmj.f5577
Comparative effectiveness of exercise and drug interventions on mortality outcomes: metaepidemiological study
Abstract
Objective: To determine the comparative effectiveness of exercise versus drug interventions on mortality outcomes.
Design: Metaepidemiological study.
Eligibility criteria: Meta-analyses of randomised controlled trials with mortality outcomes comparing the effectiveness of exercise and drug interventions with each other or with control (placebo or usual care).
Data sources: Medline and Cochrane Database of Systematic Reviews, May 2013.
Main outcome measure: Mortality.
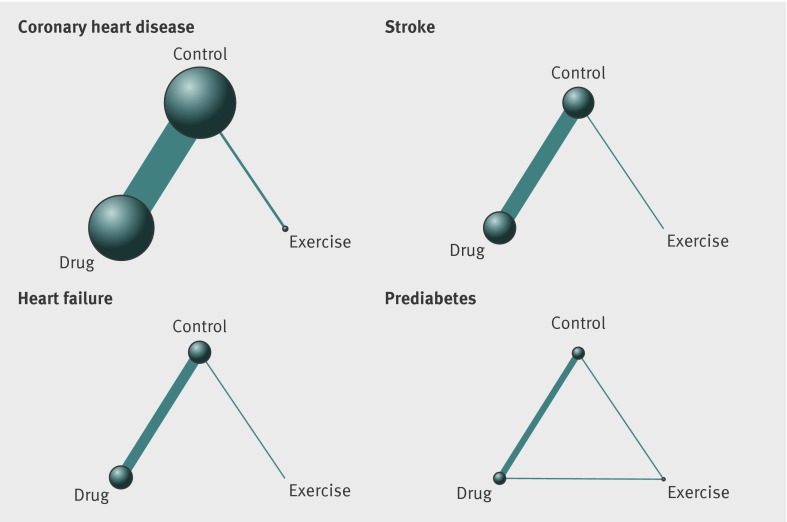
Data synthesis: We combined study level death outcomes from exercise and drug trials using random effects network meta-analysis.
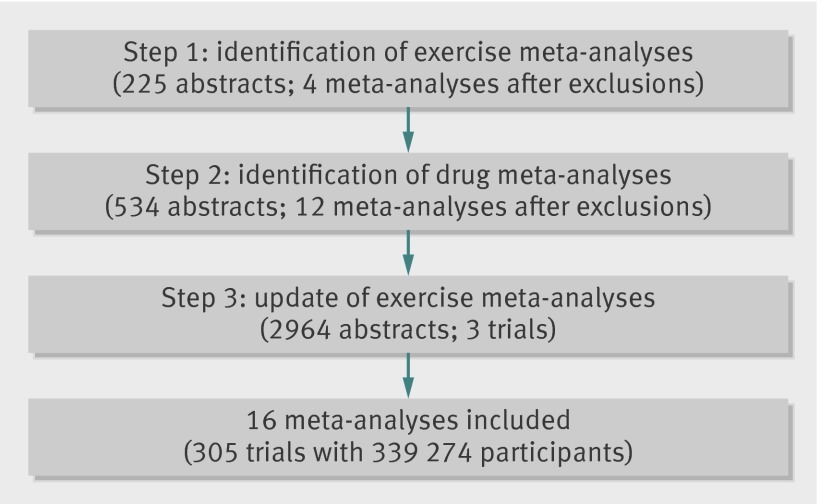
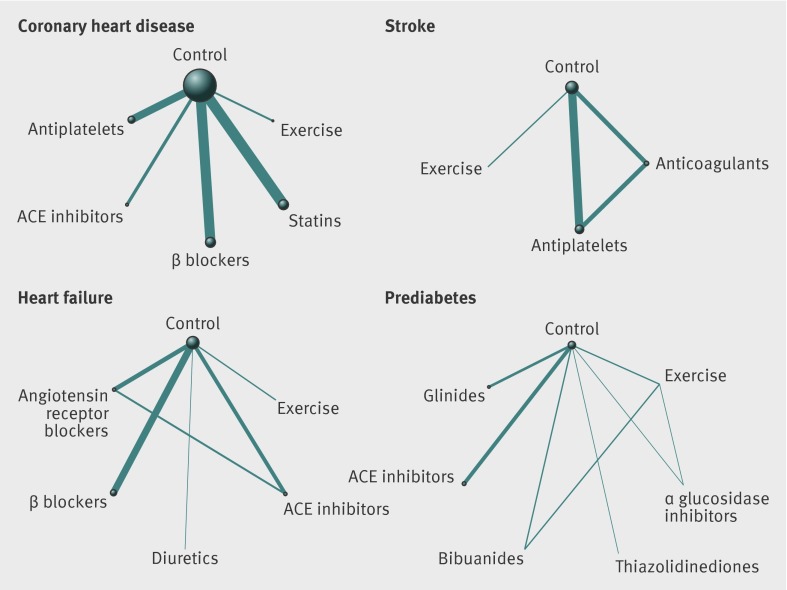
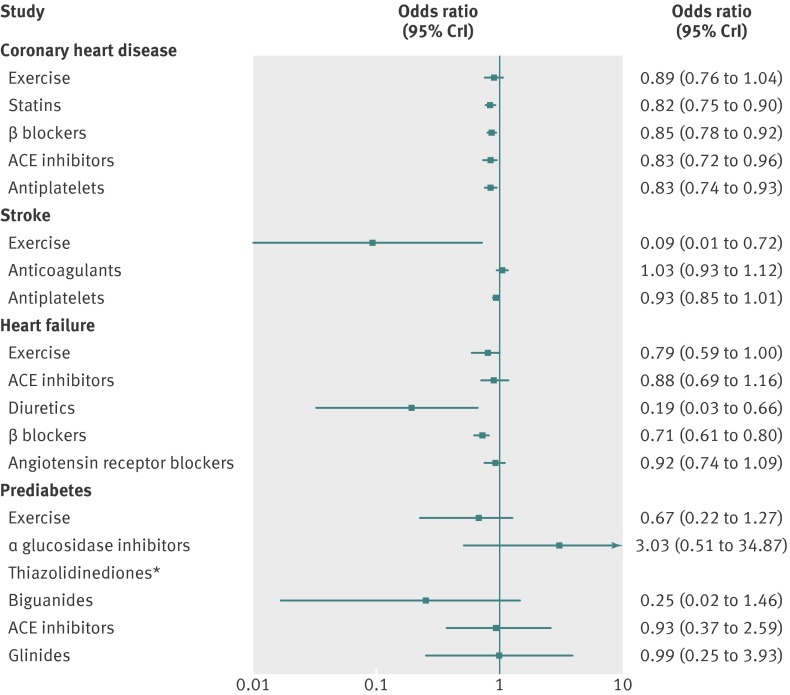
Results: We included 16 (four exercise and 12 drug) meta-analyses. Incorporating an additional three recent exercise trials, our review collectively included 305 randomised controlled trials with 339,274 participants. Across all four conditions with evidence on the effectiveness of exercise on mortality outcomes (secondary prevention of coronary heart disease, rehabilitation of stroke, treatment of heart failure, prevention of diabetes), 14,716 participants were randomised to physical activity interventions in 57 trials. No statistically detectable differences were evident between exercise and drug interventions in the secondary prevention of coronary heart disease and prediabetes. Physical activity interventions were more effective than drug treatment among patients with stroke (odds ratios, exercise v anticoagulants 0.09, 95% credible intervals 0.01 to 0.70 and exercise v antiplatelets 0.10, 0.01 to 0.62). Diuretics were more effective than exercise in heart failure (exercise v diuretics 4.11, 1.17 to 24.76). Inconsistency between direct and indirect comparisons was not significant.
Conclusions: Although limited in quantity, existing randomised trial evidence on exercise interventions suggests that exercise and many drug interventions are often potentially similar in terms of their mortality benefits in the secondary prevention of coronary heart disease, rehabilitation after stroke, treatment of heart failure, and prevention of diabetes.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
ACP Journal Club. Review: Exercise reduces mortality compared with drugs in stroke but not in CHD, HF, or prediabetes.Ann Intern Med. 2014 Apr 15;160(8):JC3. doi: 10.7326/0003-4819-160-8-201404150-02003. Ann Intern Med. 2014. PMID: 24733220 No abstract available.
References
-
- Pedersen BK, Saltin B. Evidence for prescribing exercise as therapy in chronic disease. Scand J Med Sci Sports 2006;16(S1):3-63. - PubMed
-
- Knols R, Aaronson NK, Uebelhart D, Fransen J, Aufdemkampe G. Physical exercise in cancer patients during and after medical treatment: a systematic review of randomized and controlled clinical trials. J Clin Oncol 2005;23:3830-42. - PubMed
-
- Sigal RJ, Kenny GP, Wasserman DH, Castaneda-Sceppa C, White RD. Physical activity/exercise and type 2 diabetes: a consensus statement from the American Diabetes Association. Diabetes Care 2006;29:1433-8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical