

The association of surgical margins and local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy: a meta-analysis
- PMID: 24473640
- PMCID: PMC5705035
- DOI: 10.1245/s10434-014-3480-5
The association of surgical margins and local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy: a meta-analysis
Abstract
Purpose: There is no consensus on what constitutes adequate negative margins in breast-conserving therapy (BCT). We systematically review the evidence on surgical margins in BCT for invasive breast cancer to support the development of clinical guidelines.
Methods: Study-level meta-analysis of studies reporting local recurrence (LR) data relative to final microscopic margin status and the threshold distance for negative margins. LR proportion was modeled using random-effects logistic meta-regression.
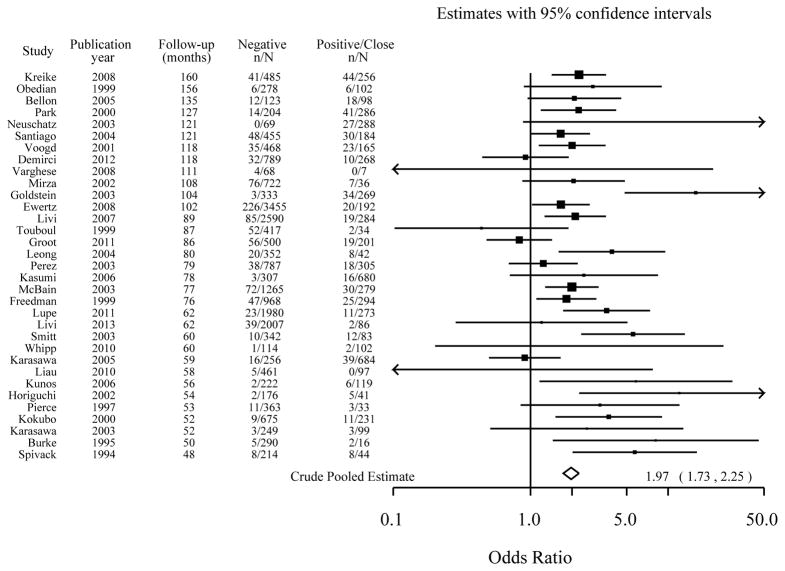
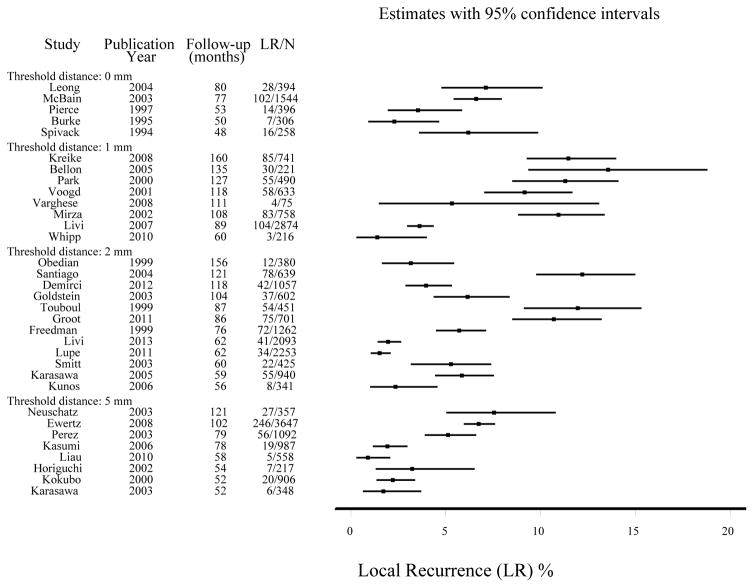
Results: Based on 33 studies (LR in 1,506 of 28,162), the odds of LR were associated with margin status [model 1: odds ratio (OR) 1.96 for positive/close vs negative; model 2: OR 1.74 for close vs. negative, 2.44 for positive vs. negative; (P < 0.001 both models)] but not with margin distance [model 1: >0 mm vs. 1 mm (referent) vs. 2 mm vs. 5 mm (P = 0.12); and model 2: 1 mm (referent) vs. 2 mm vs. 5 mm (P = 0.90)], adjusting for study median follow-up time. There was little to no statistical evidence that the odds of LR decreased as the distance for declaring negative margins increased, adjusting for follow-up time [model 1: 1 mm (OR 1.0, referent), 2 mm (OR 0.95), 5 mm (OR 0.65), P = 0.21 for trend; and model 2: 1 mm (OR 1.0, referent), 2 mm (OR 0.91), 5 mm (OR 0.77), P = 0.58 for trend]. Adjustment for covariates, such as use of endocrine therapy or median-year of recruitment, did not change the findings.
Conclusions: Meta-analysis confirms that negative margins reduce the odds of LR; however, increasing the distance for defining negative margins is not significantly associated with reduced odds of LR, allowing for follow-up time. Adoption of wider relative to narrower margin widths to declare negative margins is unlikely to have a substantial additional benefit for long-term local control in BCT.
Figures
References
-
- Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. New Engl J Med. 2002;347:1227–1232. - PubMed
-
- Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. New Engl J Med. 2002;347:1233–1241. - PubMed
-
- Van Dongen JA, Voogd AC, Fentiman IS, et al. Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 trial. Journal of the National Cancer Institute. 2000;92:1143–1150. - PubMed
-
- Poggi MM, Danforth DN, Sciuto LC, et al. Eighteen-year results in the treatment of early breast carcinoma with mastectomy versus breast conservation therapy: the National Cancer Institute Randomized Trial. Cancer. 2003;98:697–702. - PubMed
-
- Blichert-Toft M, Rose C, Andersen JA, et al. Danish randomized trial comparing breast conservation therapy with mastectomy: six years of life-table analysis. Danish Breast Cancer Cooperative Group. Journal of the National Cancer Institute Monographs. 1992;(11):19–25. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
