

Interpretation of autoantibody positivity in interstitial lung disease and lung-dominant connective tissue disease
- PMID: 24473767
- PMCID: PMC4075893
- DOI: 10.1590/S1806-37132013000600012
Interpretation of autoantibody positivity in interstitial lung disease and lung-dominant connective tissue disease
Abstract
The initial evaluation of patients with interstitial lung disease (ILD) primarily involves a comprehensive, active search for the cause. Autoantibody assays, which can suggest the presence of a rheumatic disease, are routinely performed at various referral centers. When interstitial lung involvement is the condition that allows the definitive diagnosis of connective tissue disease and the classical criteria are met, there is little debate. However, there is still debate regarding the significance, relevance, specificity, and pathophysiological role of autoimmunity in patients with predominant pulmonary involvement and only mild symptoms or formes frustes of connective tissue disease. The purpose of this article was to review the current knowledge of autoantibody positivity and to discuss its possible interpretations in patients with ILD and without clear etiologic associations, as well as to enhance the understanding of the natural history of an allegedly new disease and to describe the possible prognostic implications. We also discuss the proposition of a new term to be used in the classification of ILDs: lung-dominant connective tissue disease.
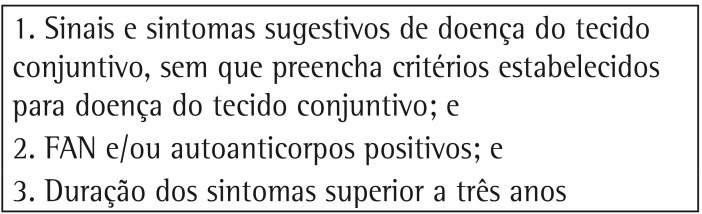
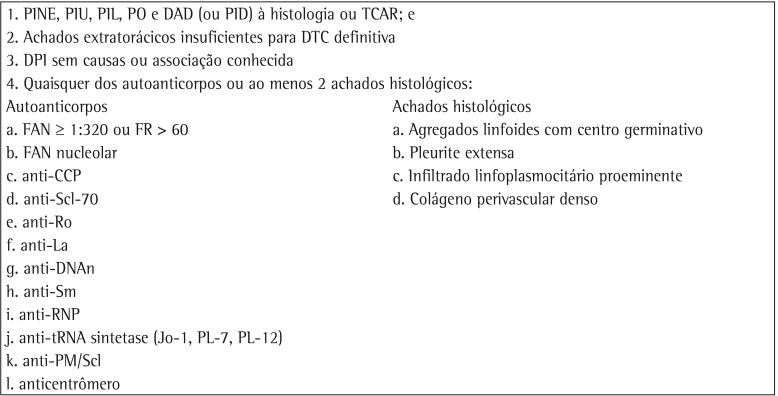
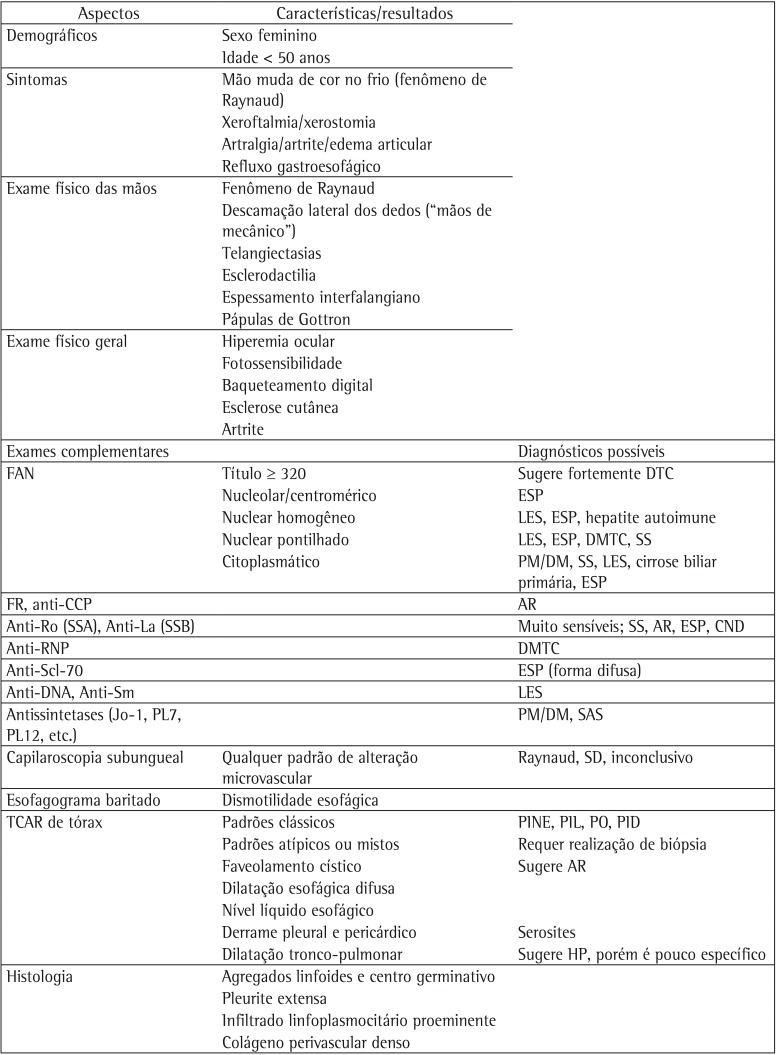
A avaliação inicial de pacientes com doença pulmonar intersticial (DPI) envolve primordialmente a busca ativa e detalhada por uma etiologia. A pesquisa rotineira de autoanticorpos é comum em diferentes centros e permite sugerir a presença de alguma doença do espectro reumatológico. Quando o acometimento pulmonar intersticial é a condição que permite o diagnóstico firmado de uma colagenose bem estabelecida, preenchendo os critérios clássicos, há pouco debate. Entretanto, ainda existe muita discussão sobre o significado, a relevância, a especificidade e o papel fisiopatológico da autoimunidade nos pacientes que tenham prioritariamente acometimento respiratório e apenas algum indício leve ou frustro de colagenose. O propósito dessa revisão foi apresentar o conhecimento atual e discutir possibilidades de interpretação da positividade de autoanticorpos em pacientes com DPI que não tenham associações etiológicas inequívocas, assim como aumentar o entendimento da história natural de uma possível nova doença e descrever possíveis implicações prognósticas. Discutimos ainda a proposição de uma nova terminologia na classificação das DPIs, a colagenose pulmão dominante.
Figures

Comment in
-
Interstitial lung disease in suggestive forms of connective tissue disease.J Bras Pneumol. 2013 Nov-Dec;39(6):641-3. doi: 10.1590/S1806-37132013000600001. J Bras Pneumol. 2013. PMID: 24473756 Free PMC article. No abstract available.
References
-
- Baldi BG, Pereira CA, Rubin AS, Santana AN, Costa AN, Carvalho CR, et al. Highlights of the Brazilian Thoracic Association guidelines for interstitial lung diseases. J Bras Pneumol. 2012;38(3):282–291. http://dx.doi.org/10.1590/S1806-37132012000300002 PMid:22782597 - DOI - PubMed
-
- Elicker B, Pereira CA, Webb R, Leslie KO. High-resolution computed tomography patterns of diffuse interstitial lung disease with clinical and pathological correlation. J Bras Pneumol. 2008;34(9):715–744. http://dx.doi.org/10.1590/S1806-37132008000900013 - DOI - PubMed
-
- Tzelepis GE, Toya SP, Moutsopoulos HM. Occult connective tissue diseases mimicking idiopathic interstitial pneumonias. Eur Respir J. 2008;31(1):11–20. http://dx.doi.org/10.1183/09031936.00060107 - DOI - PubMed
-
- Antoniou KM, Margaritopoulos G, Economidou F, Siafakas NM. Pivotal clinical dilemmas in collagen vascular diseases associated with interstitial lung involvement. Eur Respir J. 2009;33(4):882–896. http://dx.doi.org/10.1183/09031936.00152607 - DOI - PubMed
-
- Lauretis A de, Veeraraghavan S, Renzoni E. Review series: Aspects of interstitial lung disease: connective tissue disease-associated interstitial lung disease: how does it differ from IPF? How should the clinical approach differ? Chron Respir Dis. 2011;8(1):53–82. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
