

Hypopigmented mycosis fungoides: a review of its clinical features and pathophysiology
- PMID: 24474105
- PMCID: PMC3900347
- DOI: 10.1590/abd1806-4841.20132336
Hypopigmented mycosis fungoides: a review of its clinical features and pathophysiology
Abstract
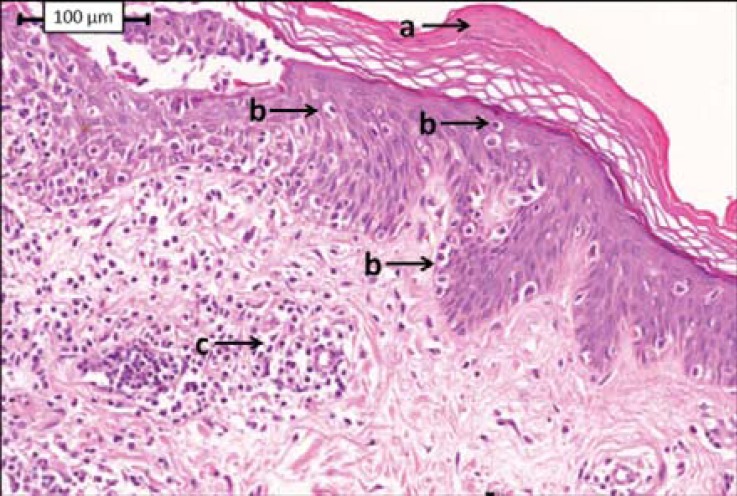
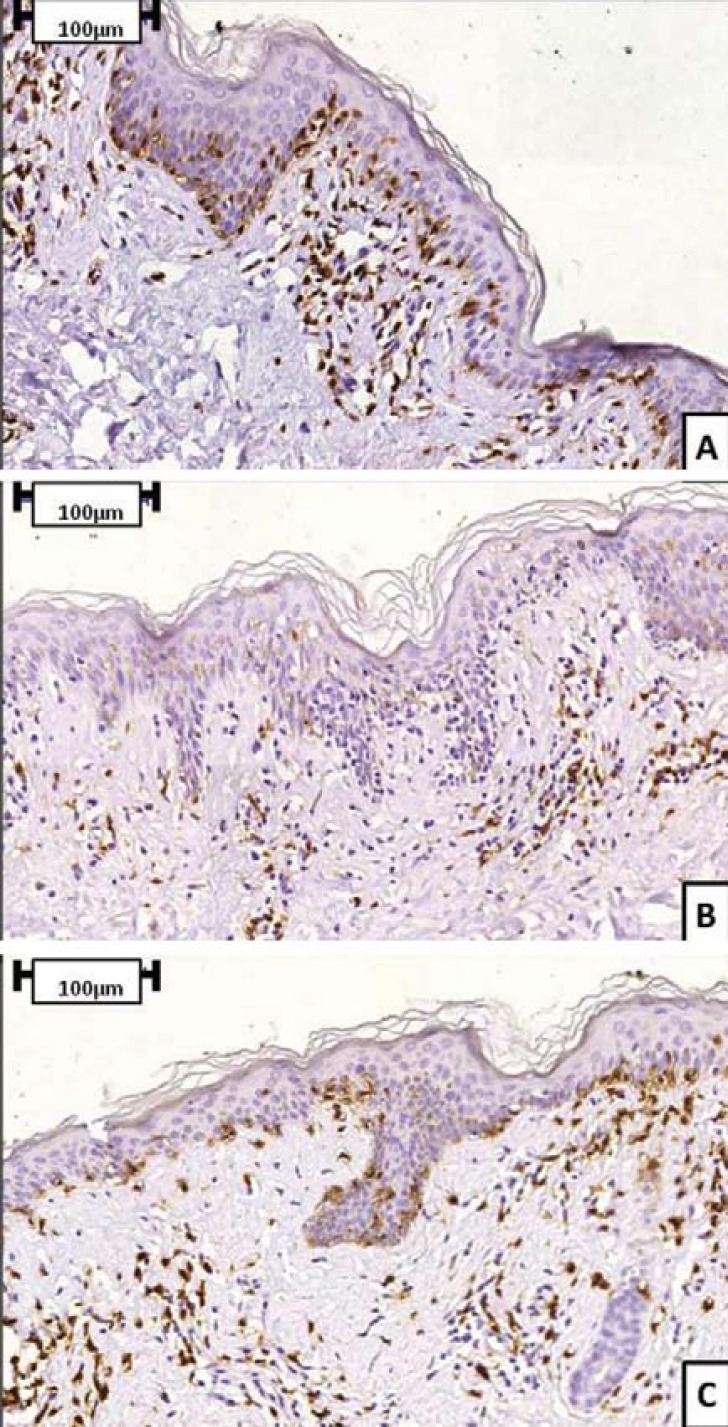
Several distinct clinical forms of mycosis fungoides have been described. Hypopigmented mycosis fungoides should be regarded as a subtype of mycosis fungoides, insofar as it presents some peculiar characteristics that contrast with the clinical features of the classical form. Most patients with hypopigmented mycosis fungoides are younger than patients typically diagnosed with classical mycosis fungoides. In addition to typical dark-skinned individuals impairment, hypopigmented mycosis fungoides has also been described in Asian patients. The prognosis for hypopigmented mycosis fungoides is much better than for classical mycosis fungoides: hypopigmented mycosis fungoides is diagnosed when there are only patches of affected skin, and lesions usually will not progress beyond terminal stages, although they can persist for many years. Diagnosis should involve clinicopathologic correlation: skin biopsy analysis often reveals intense epidermotropism, characterized by haloed, large, and atypical CD8+ lymphocytes with convoluted nuclei, in contrast to mild to moderate dermal lymphocytic infiltrate. These CD8+ cells, which participate in T helper 1-mediated immune responses, prevent evolution to mycosis fungoides plaques and tumors and could be considered the main cause of the inhibition of melanogenesis. Therefore, hypopigmentation could be considered a marker of good prognosis for mycosis fungoides.
Ultimamente diferentes formas clínicas da micose fungoide têm sido descritas. A micose fungoide hipocromiante pode ser considerada um subtipo da micose fungoide, apresentando algumas características peculiares que contrastam com os achados da forma clássica da micose fungoide. A maioria dos pacientes com micose fungoide hipocromiante são mais jovens que aqueles acometidos pela micose fungoide clássica. Esta variante é descrita principalmente em indivíduos melanodérmicos (afroamericanos e asiáticos). O prognóstico é melhor que o observado para a forma clássica: ao diagnóstico, os pacientes apresentam somente "patches", que tendem a perdurar por longos períodos, sem evolução para estágios mais avançados. O diagnóstico é feito através da correlação clinicopatológica: biópsia da lesão cutânea frequentemente revela intenso epidermotropismo, caracterizado por linfócitos CD8+ atípicos, grandes, com halo e núcleo convoluto, contrastando com o infiltrado dérmico leve a moderado. Estas células CD8+, que participam do perfil de resposta T helper-1, impediriam a evolução da doença para o desenvolvimento de placas infiltradas e tumores, além de determinar a inibição da melanogênese nas lesões hipocrômicas. Portanto, a hipocromia poderia ser considerada um marcador de bom prognóstico na micose fungoide.
Conflict of interest statement
Conflict of interest: None
Figures



Similar articles
-
Hypopigmented Mycosis Fungoides: A Clinical and Histopathology Analysis in 9 Children.Am J Dermatopathol. 2021 Apr 1;43(4):259-265. doi: 10.1097/DAD.0000000000001723. Am J Dermatopathol. 2021. PMID: 33201017
-
[Mycosis fungoides in children and adolescents: a report of six cases with predominantly hypopigmentation, along with a literature review].Dermatol Online J. 2012 Mar 15;18(3):5. Dermatol Online J. 2012. PMID: 22483516 Review. Portuguese.
-
Hypopigmented mycosis fungoides versus mycosis fungoides with concomitant hypopigmented lesions: same disease or different variants of mycosis fungoides?Dermatology. 2014;229(3):271-4. doi: 10.1159/000363319. Epub 2014 Oct 11. Dermatology. 2014. PMID: 25323446
-
Vitiligo vs. hypopigmented mycosis fungoides (histopathological and immunohistochemical study, univariate analysis).Eur J Dermatol. 2006 Jan-Feb;16(1):17-22. Eur J Dermatol. 2006. PMID: 16436337
-
Hypopigmented mycosis fungoides: a retrospective clinicohistopathologic study.J Eur Acad Dermatol Venereol. 2017 May;31(5):808-814. doi: 10.1111/jdv.13843. Epub 2016 Aug 12. J Eur Acad Dermatol Venereol. 2017. PMID: 27515575 Review.
Cited by
-
Childhood hypopigmented mycosis fungoides: a commonly delayed diagnosis.BMJ Case Rep. 2014 Dec 23;2014:bcr2014208306. doi: 10.1136/bcr-2014-208306. BMJ Case Rep. 2014. PMID: 25538219 Free PMC article.
-
Post-Inflammatory Hypopigmentation: Review of the Etiology, Clinical Manifestations, and Treatment Options.J Clin Med. 2023 Feb 3;12(3):1243. doi: 10.3390/jcm12031243. J Clin Med. 2023. PMID: 36769891 Free PMC article. Review.
-
An illustrative case of hypopigmented mycosis fungoides.SAGE Open Med Case Rep. 2025 Jul 31;13:2050313X251359024. doi: 10.1177/2050313X251359024. eCollection 2025. SAGE Open Med Case Rep. 2025. PMID: 40756744 Free PMC article.
-
A Comprehensive Update of the Atypical, Rare and Mimicking Presentations of Mycosis Fungoides.Dermatol Ther (Heidelb). 2021 Dec;11(6):1931-1951. doi: 10.1007/s13555-021-00625-6. Epub 2021 Oct 28. Dermatol Ther (Heidelb). 2021. PMID: 34709600 Free PMC article. Review.
-
Paediatric cutaneous lymphomas including rare subtypes: A 40-year experience at a tertiary referral centre.J Eur Acad Dermatol Venereol. 2025 Jan;39(1):161-170. doi: 10.1111/jdv.20028. Epub 2024 Apr 23. J Eur Acad Dermatol Venereol. 2025. PMID: 38650545 Free PMC article.
References
-
- Criscione VD, Weinstock MA. Incidence of cutaneous T-cell lymphoma in the United States, 1973-2002. Arch Dermatol. 2007;143:854–859. - PubMed
-
- Keehn CA, Belongie IP, Shistik G, Fenske NA, Glass LF. The diagnosis, staging, and treatment options for mycosis fungoides. Cancer Control. 2007;14:102–111. - PubMed
-
- FestaNeto C, Sanches JA, Melotti CZ. Lymphoproliferative processes of the skin. Part 2 - Cutaneous T-cell and NK-cell lymphomas. An Bras Dermatol. 2006;87:7–25.
-
- Ackerman AB, Miller RC, Shapiro L. Pustular mycosis fungoides. Arch Dermatol. 1966;93:221–225. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials