

Risk factors for pancreatic cancer: underlying mechanisms and potential targets
- PMID: 24474939
- PMCID: PMC3893685
- DOI: 10.3389/fphys.2013.00415
Risk factors for pancreatic cancer: underlying mechanisms and potential targets
Abstract
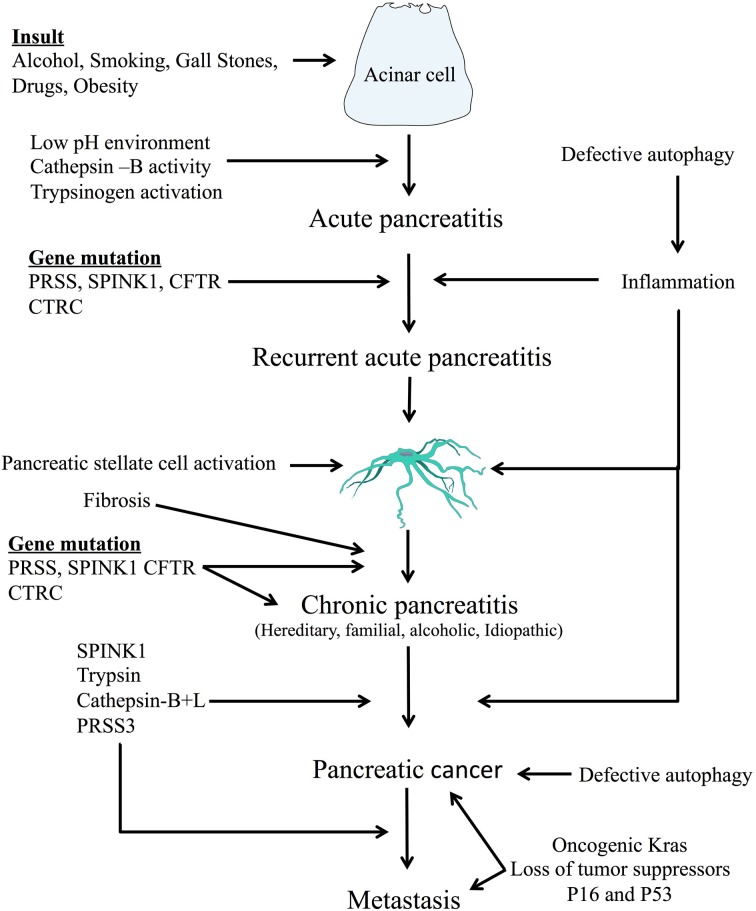
Purpose of the review: Pancreatic cancer is extremely aggressive, forming highly chemo-resistant tumors, and has one of the worst prognoses. The evolution of this cancer is multi-factorial. Repeated acute pancreatic injury and inflammation are important contributing factors in the development of pancreatic cancer. This article attempts to understand the common pathways linking pancreatitis to pancreatic cancer.
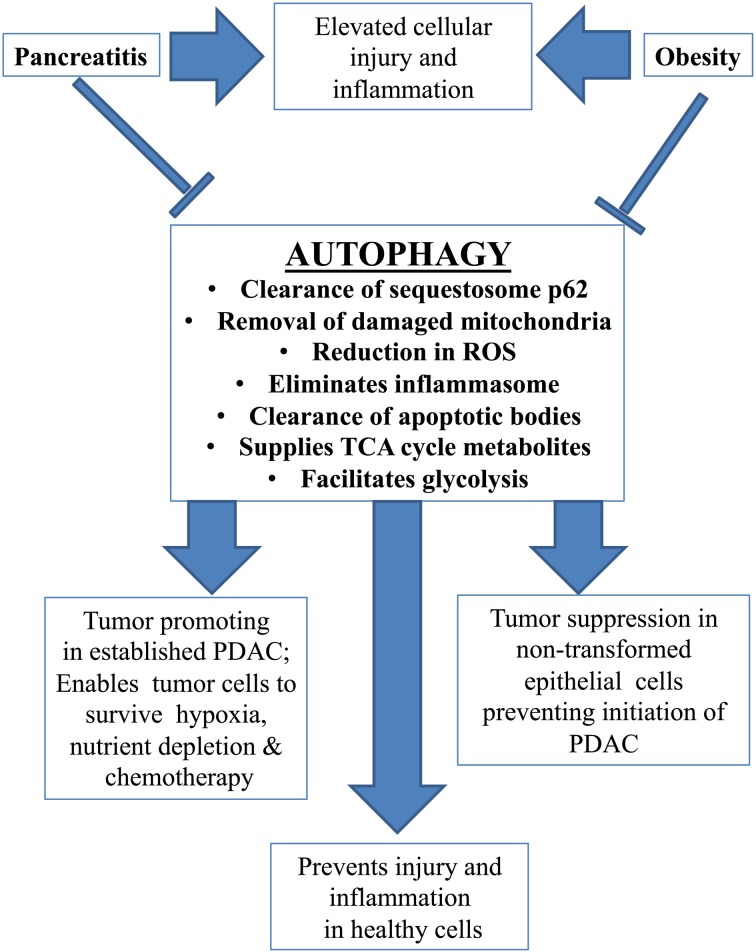
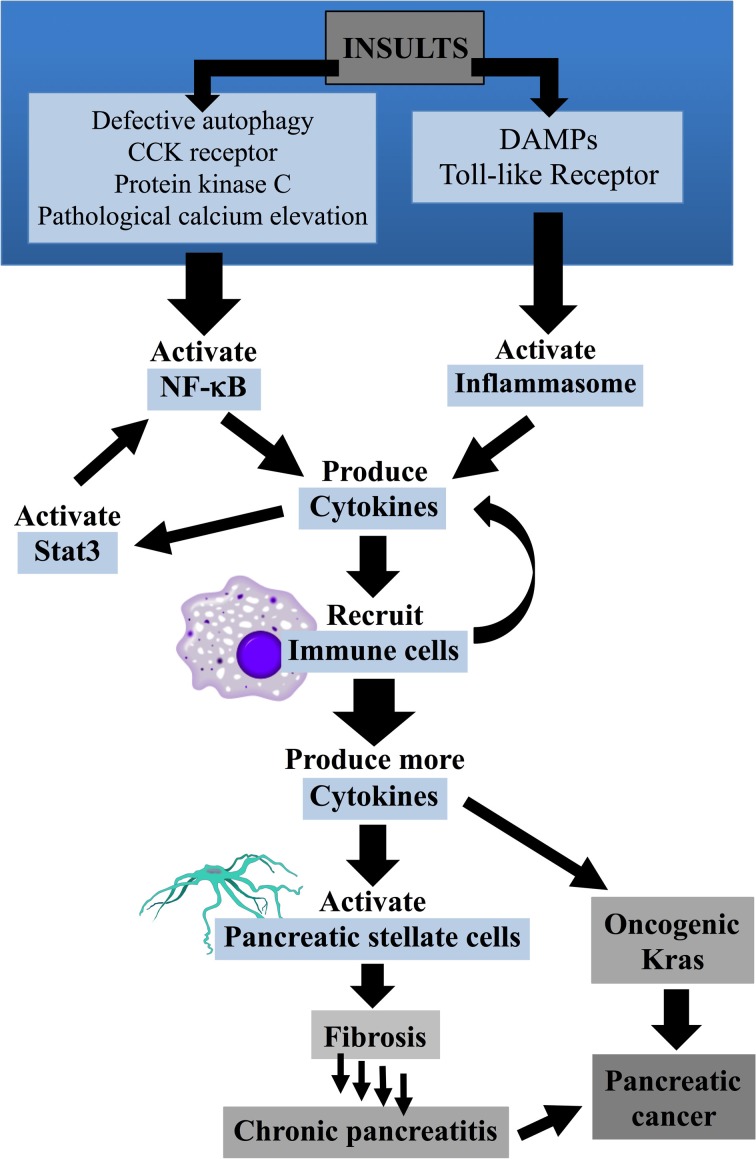
Recent findings: Intracellular activation of both pancreatic enzymes and the transcription factor NF-κB are important mechanisms that induce acute pancreatitis (AP). Recurrent pancreatic injury due to genetic susceptibility, environmental factors such as smoking, alcohol intake, and conditions such as obesity lead to increases in oxidative stress, impaired autophagy and constitutive activation of inflammatory pathways. These processes can stimulate pancreatic stellate cells, thereby increasing fibrosis and encouraging chronic disease development. Activation of oncogenic Kras mutations through inflammation, coupled with altered levels of tumor suppressor proteins (p53 and p16) can ultimately lead to development of pancreatic cancer.
Summary: Although our understanding of pancreatitis and pancreatic cancer has tremendously increased over many years, much remains to be elucidated in terms of common pathways linking these conditions.
Keywords: K-ras; autophagy; inflammation; pancreatic cancer; pancreatitis; stellate cells.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous