

Frequent seizures are associated with a network of gray matter atrophy in temporal lobe epilepsy with or without hippocampal sclerosis
- PMID: 24475055
- PMCID: PMC3903486
- DOI: 10.1371/journal.pone.0085843
Frequent seizures are associated with a network of gray matter atrophy in temporal lobe epilepsy with or without hippocampal sclerosis
Abstract
Objective: Patients with temporal lobe epilepsy (TLE) with hippocampal sclerosis (HS) have diffuse subtle gray matter (GM) atrophy detectable by MRI quantification analyses. However, it is not clear whether the etiology and seizure frequency are associated with this atrophy. We aimed to evaluate the occurrence of GM atrophy and the influence of seizure frequency in patients with TLE and either normal MRI (TLE-NL) or MRI signs of HS (TLE-HS).
Methods: We evaluated a group of 172 consecutive patients with unilateral TLE-HS or TLE-NL as defined by hippocampal volumetry and signal quantification (122 TLE-HS and 50 TLE-NL) plus a group of 82 healthy individuals. Voxel-based morphometry was performed with VBM8/SPM8 in 3T MRIs. Patients with up to three complex partial seizures and no generalized tonic-clonic seizures in the previous year were considered to have infrequent seizures. Those who did not fulfill these criteria were considered to have frequent seizures.
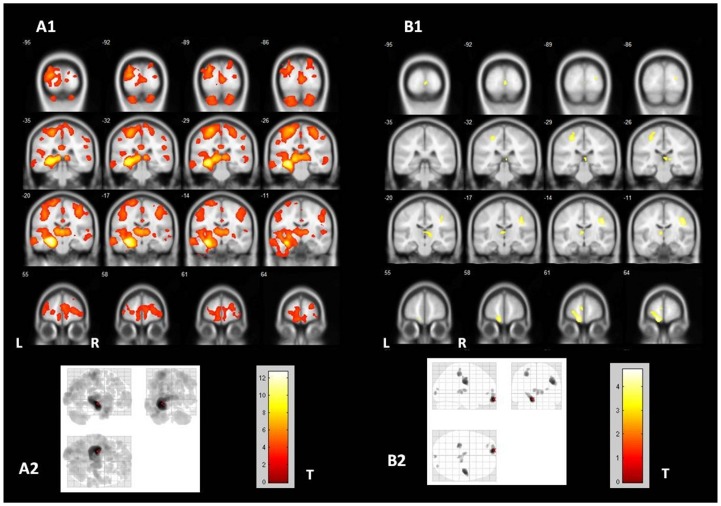
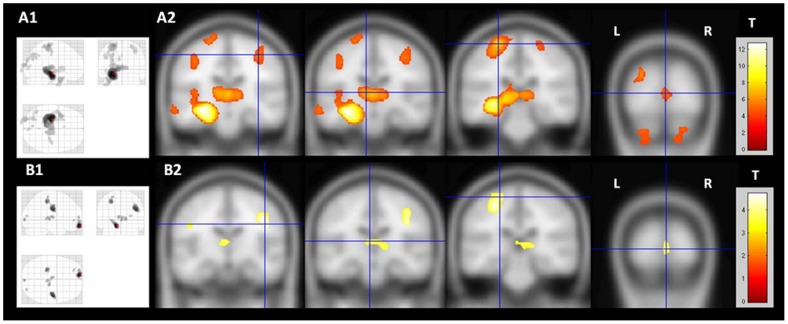
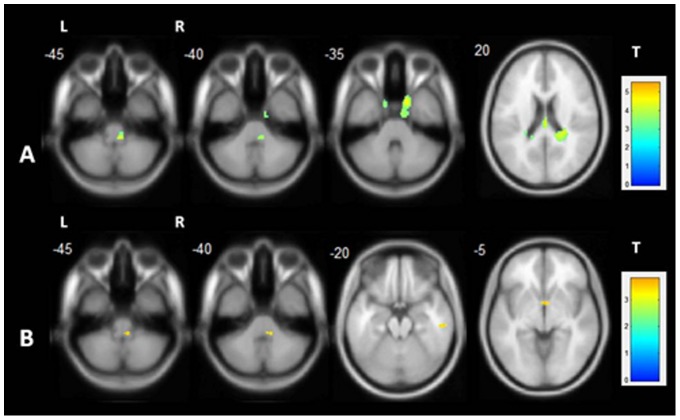
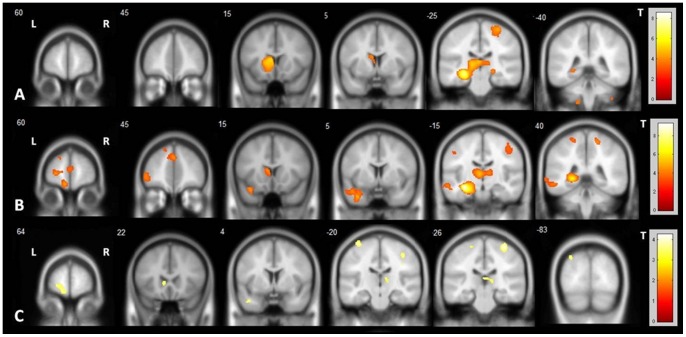
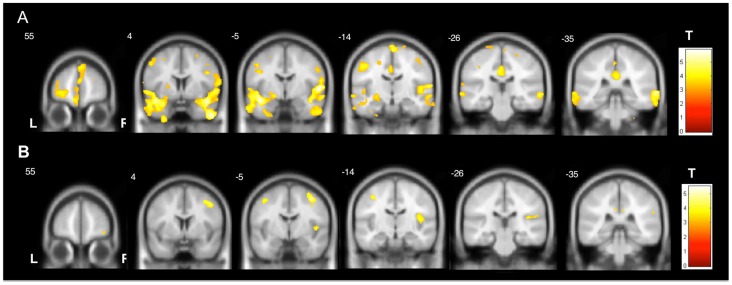
Results: Patients with TLE-HS had more pronounced GM atrophy, including the ipsilateral mesial temporal structures, temporal lobe, bilateral thalami and pre/post-central gyri. Patients with TLE-NL had more subtle GM atrophy, including the ipsilateral orbitofrontal cortex, bilateral thalami and pre/post-central gyri. Both TLE-HS and TLE-NL showed increased GM volume in the contralateral pons. TLE-HS patients with frequent seizures had more pronounced GM atrophy in extra-temporal regions than TLE-HS with infrequent seizures. Patients with TLE-NL and infrequent seizures had no detectable GM atrophy. In both TLE-HS and TLE-NL, the duration of epilepsy correlated with GM atrophy in extra-hippocampal regions.
Conclusion: Although a diffuse network GM atrophy occurs in both TLE-HS and TLE-NL, this is strikingly more evident in TLE-HS and in patients with frequent seizures. These findings suggest that neocortical atrophy in TLE is related to the ongoing seizures and epilepsy duration, while thalamic atrophy is more probably related to the original epileptogenic process.
Conflict of interest statement
Figures
References
-
- Bonilha L, Rorden C, Castellano G, Pereira F, Rio PA, et al. (2004) Voxel-based morphometry reveals gray matter network atrophy in refractory medial temporal lobe epilepsy. Arch Neurol 61: 1379–1384. - PubMed
-
- Spencer SS (2002) Neural networks in human epilepsy: Evidence of and implications for treatment. Epilepsia 43: 219–227. - PubMed
-
- Hauser WA (1992) The natural history of temporal lobe epilepsy. In: Lüders, H.O., ed. Epilepsy Surgery. New York: Raven Press, p. 133–141.
-
- Cohen-Gadol AA, Bradley CC, Williamson A, Kim JH, Westerveld M, et al. (2005) Normal magnetic resonance imaging and medial temporal lobe epilepsy: the clinical syndrome of paradoxical temporal lobe epilepsy. J Neurosurg 102: 902–909. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
