

Biomarkers and molecular analysis to improve bloodstream infection diagnostics in an emergency care unit
- PMID: 24475269
- PMCID: PMC3903623
- DOI: 10.1371/journal.pone.0087315
Biomarkers and molecular analysis to improve bloodstream infection diagnostics in an emergency care unit
Abstract
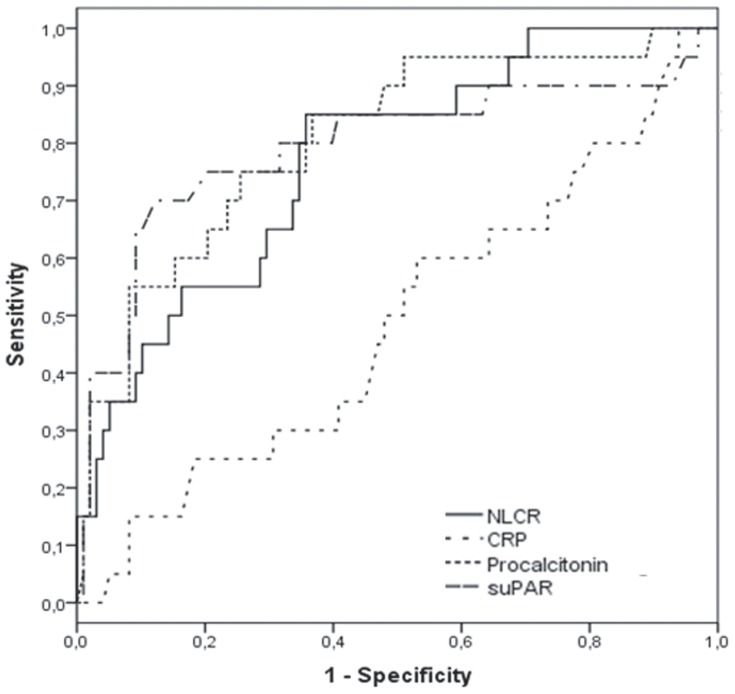
Molecular pathogen detection from blood is still expensive and the exact clinical value remains to be determined. The use of biomarkers may assist in preselecting patients for immediate molecular testing besides blood culture. In this study, 140 patients with ≥ 2 SIRS criteria and clinical signs of infection presenting at the emergency department of our hospital were included. C-reactive protein (CRP), neutrophil-lymphocyte count ratio (NLCR), procalcitonin (PCT) and soluble urokinase plasminogen activator receptor (suPAR) levels were determined. One ml EDTA blood was obtained and selective pathogen DNA isolation was performed with MolYsis (Molzym). DNA samples were analysed for the presence of pathogens, using both the MagicPlex Sepsis Test (Seegene) and SepsiTest (Molzym), and results were compared to blood cultures. Fifteen patients had to be excluded from the study, leaving 125 patients for further analysis. Of the 125 patient samples analysed, 27 presented with positive blood cultures of which 7 were considered to be contaminants. suPAR, PCT, and NLCR values were significantly higher in patients with positive blood cultures compared to patients without (p < 0.001). Receiver operating characteristic curves of the 4 biomarkers for differentiating bacteremia from non-bacteremia showed the highest area under the curve (AUC) for PCT (0.806 (95% confidence interval 0.699-0.913)). NLCR, suPAR and CRP resulted in an AUC of 0.770, 0.793, and 0.485, respectively. When compared to blood cultures, the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for SepsiTest and MagicPlex Sepsis Test were 11%, 96%, 43%, 80%, and 37%, 77%, 30%, 82%, respectively. In conclusion, both molecular assays perform poorly when one ml whole blood is used from emergency care unit patients. NLCR is a cheap, fast, easy to determine, and rapidly available biomarker, and therefore seems most promising in differentiating BSI from non-BSI patients for subsequent pathogen identification using molecular diagnostics.
Conflict of interest statement
Figures
Similar articles
-
Diagnostic accuracy of soluble urokinase plasminogen activator receptor (suPAR) for prediction of bacteremia in patients with systemic inflammatory response syndrome.Clin Biochem. 2013 Feb;46(3):225-9. doi: 10.1016/j.clinbiochem.2012.11.004. Epub 2012 Nov 13. Clin Biochem. 2013. PMID: 23159293
-
The diagnostic value of soluble urokinase plasminogen activator receptor (suPAR) compared to C-reactive protein (CRP) and procalcitonin (PCT) in children with systemic inflammatory response syndrome (SIRS).J Infect Chemother. 2017 Jan;23(1):17-22. doi: 10.1016/j.jiac.2016.08.015. Epub 2016 Oct 19. J Infect Chemother. 2017. PMID: 27771157
-
Procalcitonin fails to predict bacteremia in SIRS patients: a cohort study.Int J Clin Pract. 2014 Oct;68(10):1278-81. doi: 10.1111/ijcp.12474. Epub 2014 Jun 4. Int J Clin Pract. 2014. PMID: 24898888
-
suPAR as a prognostic biomarker in sepsis.BMC Med. 2012 Jan 5;10:2. doi: 10.1186/1741-7015-10-2. BMC Med. 2012. PMID: 22221662 Free PMC article. Review.
-
The Diagnostic and Prognostic Value of suPAR in Patients with Sepsis: A Systematic Review and Meta-Analysis.Shock. 2020 Apr;53(4):416-425. doi: 10.1097/SHK.0000000000001434. Shock. 2020. PMID: 31490358 Free PMC article.
Cited by
-
NLR, MLR, PLR and RDW to predict outcome and differentiate between viral and bacterial pneumonia in the intensive care unit.Sci Rep. 2022 Sep 24;12(1):15974. doi: 10.1038/s41598-022-20385-3. Sci Rep. 2022. PMID: 36153405 Free PMC article.
-
Clinical evaluation of commercial nucleic acid amplification tests in patients with suspected sepsis.BMC Infect Dis. 2015 Apr 28;15:199. doi: 10.1186/s12879-015-0938-4. BMC Infect Dis. 2015. PMID: 25928122 Free PMC article.
-
Early prediction of blood stream infection in a prospectively collected cohort.BMC Infect Dis. 2021 Apr 2;21(1):316. doi: 10.1186/s12879-021-05990-3. BMC Infect Dis. 2021. PMID: 33810788 Free PMC article.
-
Current Status of Antibiotic Stewardship and the Role of Biomarkers in Antibiotic Stewardship Programs.Infect Chemother. 2022 Dec;54(4):674-698. doi: 10.3947/ic.2022.0172. Infect Chemother. 2022. PMID: 36596680 Free PMC article. Review.
-
The Current Status of Genes and Genetic Testing in Emergency Medicine: A Narrative Review.Adv J Emerg Med. 2019 Aug 25;4(1):e10. doi: 10.22114/ajem.v0i0.216. eCollection 2020 Winter. Adv J Emerg Med. 2019. PMID: 31938779 Free PMC article. Review.
References
-
- Emonet S, Schrenzel J (2011) How could rapid bacterial identification improve the management of septic patients? Expert Rev Anti Infect Ther 9: 707–709. - PubMed
-
- Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, et al. (2006) Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 34: 1589–1596. - PubMed
-
- Vincent JL (2008) Clinical sepsis and septic shock—definition, diagnosis and management principles. Langenbecks Arch Surg 393: 817–824. - PubMed
-
- Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, et al. (1992) Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 101: 1644–1655. - PubMed
-
- Grace CJ, Lieberman J, Pierce K, Littenberg B (2001) Usefulness of blood culture for hospitalized patients who are receiving antibiotic therapy. Clin Infect Dis 32: 1651–1655. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
