

Bone metastases in castration-resistant prostate cancer: associations between morphologic CT patterns, glycolytic activity, and androgen receptor expression on PET and overall survival
- PMID: 24475817
- PMCID: PMC4263648
- DOI: 10.1148/radiol.13130625
Bone metastases in castration-resistant prostate cancer: associations between morphologic CT patterns, glycolytic activity, and androgen receptor expression on PET and overall survival
Abstract
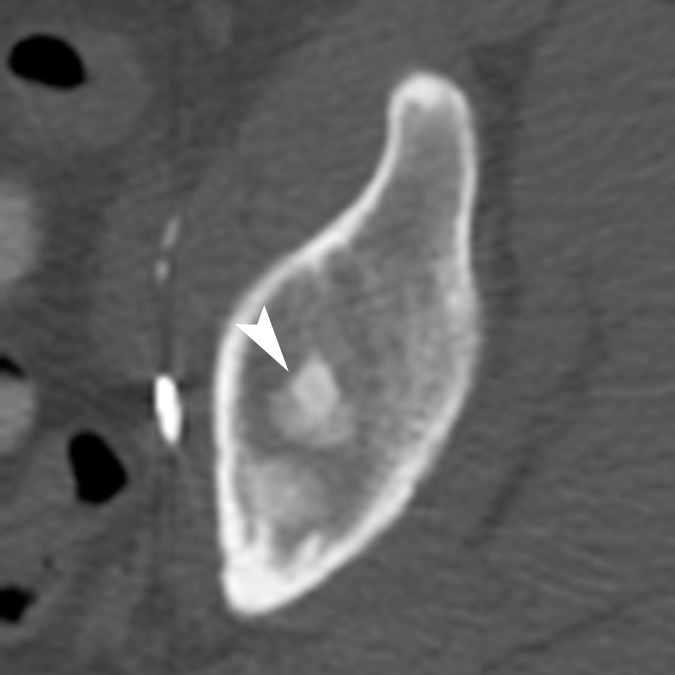
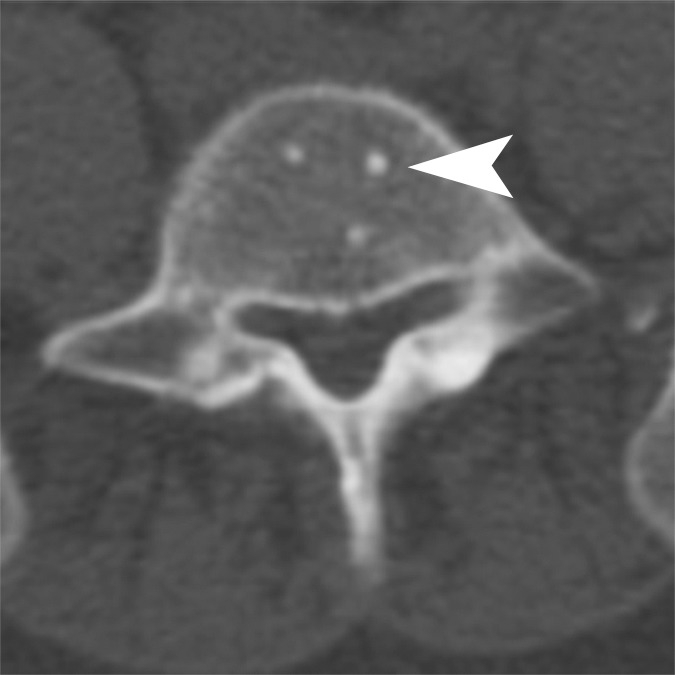
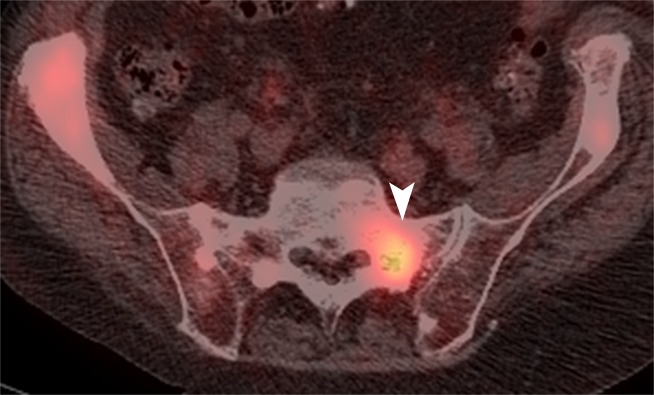
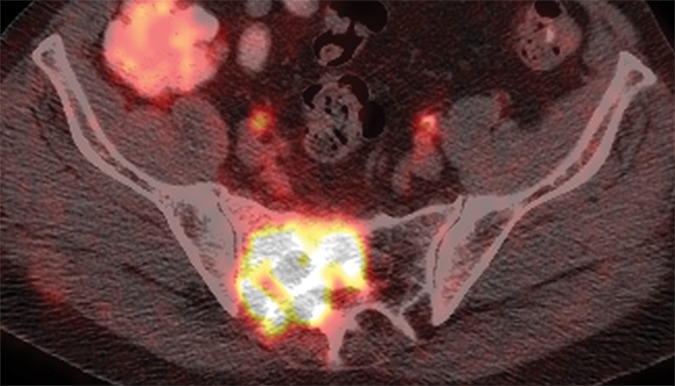
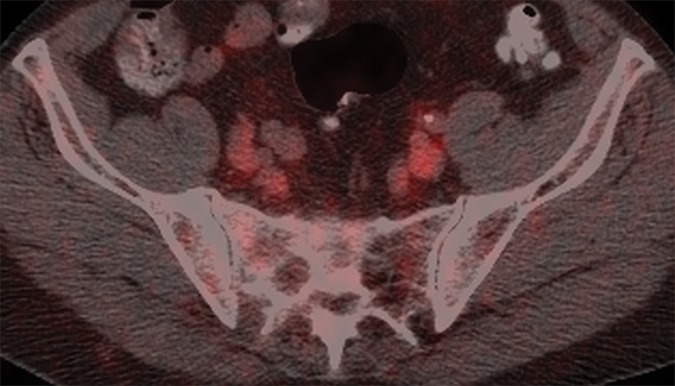
Purpose: To compare the features of bone metastases at computed tomography (CT) to tracer uptake at fluorine 18 fluorodeoxyglucose (FDG) positron emission tomography (PET) and fluorine 18 16β-fluoro-5-dihydrotestosterone (FDHT) PET and to determine associations between these imaging features and overall survival in men with castration-resistant prostate cancer.
Materials and methods: This is a retrospective study of 38 patients with castration-resistant prostate cancer. Two readers independently evaluated CT, FDG PET, and FDHT PET features of bone metastases. Associations between imaging findings and overall survival were determined by using univariate Cox proportional hazards regression.
Results: In 38 patients, reader 1 detected 881 lesions and reader 2 detected 867 lesions. Attenuation coefficients at CT correlated inversely with FDG (reader 1: r = -0.3007; P < .001; reader 2: r = -0.3147; P < .001) and FDHT (reader 1: r = -0.2680; P = .001; reader 2: r = -0.3656; P < .001) uptake. The number of lesions on CT scans was significantly associated with overall survival (reader 1: hazard ratio [HR], 1.025; P = .05; reader 2: HR, 1.021; P = .04). The numbers of lesions on FDG and FDHT PET scans were significantly associated with overall survival for reader 1 (HR, 1.051-1.109; P < .001) and reader 2 (HR, 1.026-1.082; P ≤ .009). Patients with higher FDHT uptake (lesion with the highest maximum standardized uptake value) had significantly shorter overall survival (reader 1: HR, 1.078; P = .02; reader 2: HR, 1.092; P = .02). FDG uptake intensity was not associated with overall survival (reader 1, P = .65; reader 2, P = .38).
Conclusion: In patients with castration-resistant prostate cancer, numbers of bone lesions on CT, FDG PET, and FDHT PET scans and the intensity of FDHT uptake are significantly associated with overall survival.
RSNA, 2013
Figures













Comment in
-
Association of overall survival with glycolytic activity of castrate-resistant prostate cancer metastases.Radiology. 2015 Feb;274(2):624-5. doi: 10.1148/radiol.14141593. Radiology. 2015. PMID: 25625748 No abstract available.
-
Response.Radiology. 2015 Feb;274(2):625. Radiology. 2015. PMID: 25785291 No abstract available.
References
-
- Scher HI, Fizazi K, Saad F, et al. . Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med 2012;367(13):1187–1197. - PubMed
-
- Larson SM, Morris M, Gunther I, et al. . Tumor localization of 16beta-18F-fluoro-5alpha-dihydrotestosterone versus 18F-FDG in patients with progressive, metastatic prostate cancer. J Nucl Med 2004;45(3):366–373. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
