

Screen or not to screen for peripheral arterial disease: guidance from a decision model
- PMID: 24476213
- PMCID: PMC3912926
- DOI: 10.1186/1471-2458-14-89
Screen or not to screen for peripheral arterial disease: guidance from a decision model
Abstract
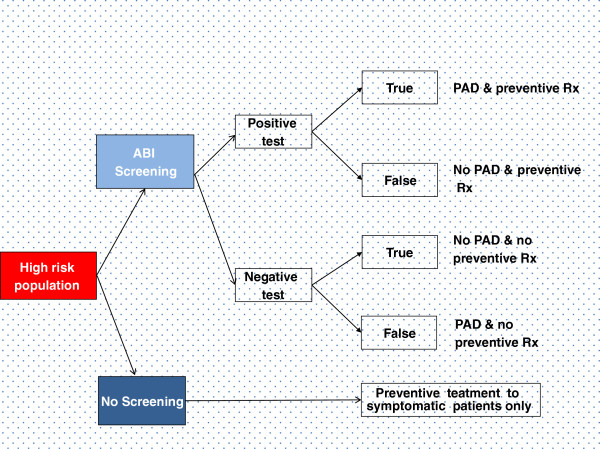
Background: Asymptomatic Peripheral Arterial Disease (PAD) is associated with greater risk of acute cardiovascular events. This study aims to determine the cost-effectiveness of one time only PAD screening using Ankle Brachial Index (ABI) test and subsequent anti platelet preventive treatment (low dose aspirin or clopidogrel) in individuals at high risk for acute cardiovascular events compared to no screening and no treatment using decision analytic modelling.
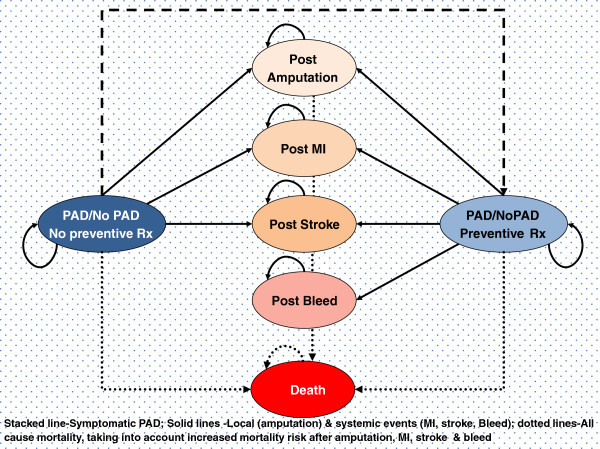
Methods: A probabilistic Markov model was developed to evaluate the life time cost-effectiveness of the strategy of selective PAD screening and consequent preventive treatment compared to no screening and no preventive treatment. The analysis was conducted from the Dutch societal perspective and to address decision uncertainty, probabilistic sensitivity analysis was performed. Results were based on average values of 1000 Monte Carlo simulations and using discount rates of 1.5% and 4% for effects and costs respectively. One way sensitivity analyses were performed to identify the two most influential model parameters affecting model outputs. Then, a two way sensitivity analysis was conducted for combinations of values tested for these two most influential parameters.
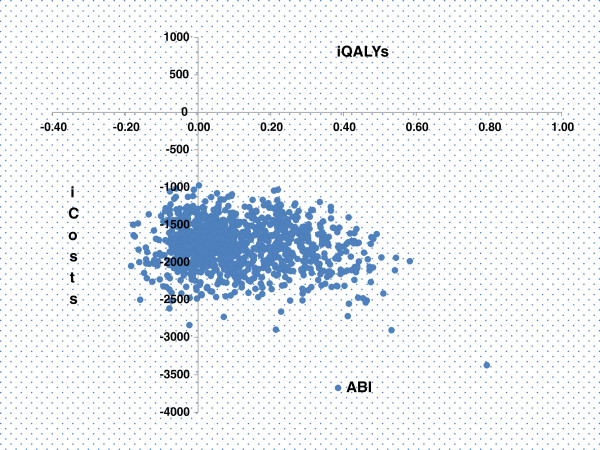
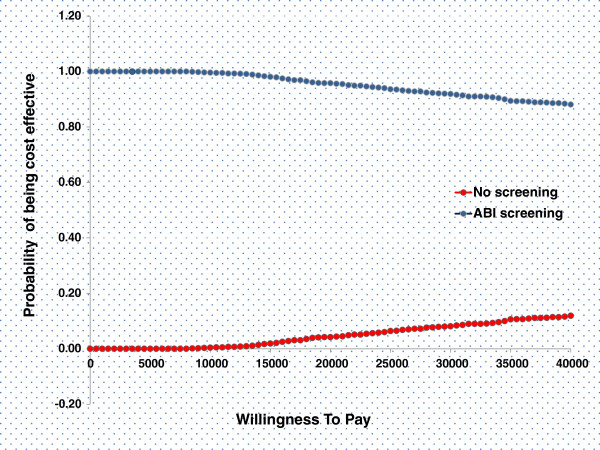
Results: For the PAD screening strategy, life years and quality adjusted life years gained were 21.79 and 15.66 respectively at a lifetime cost of 26,548 Euros. Compared to no screening and treatment (20.69 life years, 15.58 Quality Adjusted Life Years, 28,052 Euros), these results indicate that PAD screening and treatment is a dominant strategy. The cost effectiveness acceptability curves show 88% probability of PAD screening being cost effective at the Willingness To Pay (WTP) threshold of 40000 Euros. In a scenario analysis using clopidogrel as an alternative anti-platelet drug, PAD screening strategy remained dominant.
Conclusion: This decision analysis suggests that targeted ABI screening and consequent secondary prevention of cardiovascular events using low dose aspirin or clopidogrel in the identified patients is a cost-effective strategy. Implementation of targeted PAD screening and subsequent treatment in primary care practices and in public health programs is likely to improve the societal health and to save health care costs by reducing catastrophic cardiovascular events.
Figures
References
-
- Criqui MH, Denenberg JO. The generalized nature of atherosclerosis: how peripheral arterial disease may predict adverse events from coronary artery disease. Vasc Med. 1998;3(3):241–245. - PubMed
-
- McDermott MM, Liu K, Greenland P, Guralnik JM, Criqui MH, Chan C, Pearce WH, Schneider JR, Ferrucci L, Celic L. et al. Functional decline in peripheral arterial disease: associations with the ankle brachial index and leg symptoms. Jama. 2004;292(4):453–461. doi: 10.1001/jama.292.4.453. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
