

Evaluation of Barrett esophagus by multiphoton microscopy
- PMID: 24476518
- PMCID: PMC4089503
- DOI: 10.5858/arpa.2012-0675-OA
Evaluation of Barrett esophagus by multiphoton microscopy
Erratum in
- Arch Pathol Lab Med. 2014 May;138(5):582
Abstract
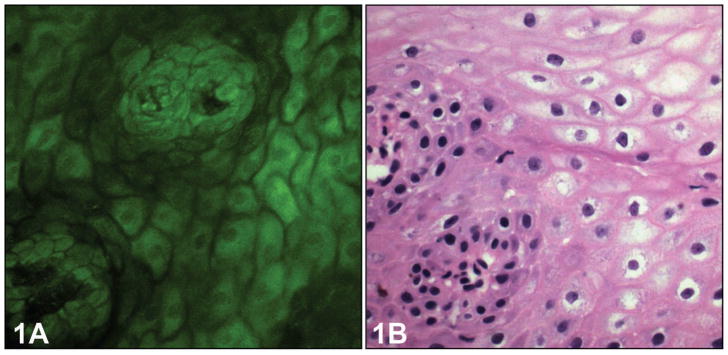
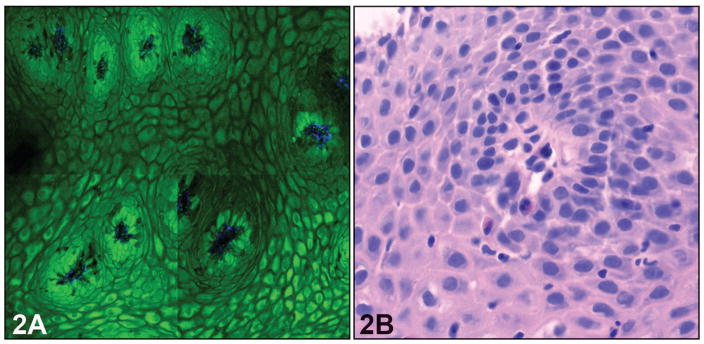
Context: Multiphoton microscopy (MPM) based on 2-photon excitation fluorescence and second-harmonic generation allows simultaneous visualization of cellular details and extracellular matrix components of fresh, unfixed, and unstained tissue. Portable multiphoton microscopes, which could be placed in endoscopy suites, and multiphoton endomicroscopes are in development, but their clinical utility is unknown.
Objective: To examine fresh, unfixed endoscopic biopsies obtained from the distal esophagus and gastroesophageal junction to (1) define the MPM characteristics of normal esophageal squamous mucosa and gastric columnar mucosa, and (2) evaluate whether diagnosis of intestinal metaplasia/Barrett esophagus (BE) could be made reliably with MPM.
Design: The study examined 35 untreated, fresh biopsy specimens from 25 patients who underwent routine upper endoscopy. A Zeiss LSM 710 Duo microscope (Carl Zeiss, Thornwood, New York) coupled to a Spectra-Physics (Mountain View, California) Tsunami Ti:sapphire laser was used to obtain a MPM image within 4 hours of fresh specimen collection. After obtaining MPM images, the biopsy specimens were placed in 10% buffered formalin and submitted for routine histopathologic examination. Then, the MPM images were compared with the findings in the hematoxylin-eosin-stained, formalin-fixed, paraffin-embedded sections. The MPM characteristics of the squamous, gastric-type columnar and intestinal-type columnar epithelium were analyzed. In biopsies with discrepancy between MPM imaging and hematoxylin-eosin-stained sections, the entire tissue block was serially sectioned and reevaluated. A diagnosis of BE was made when endoscopic and histologic criteria were satisfied.
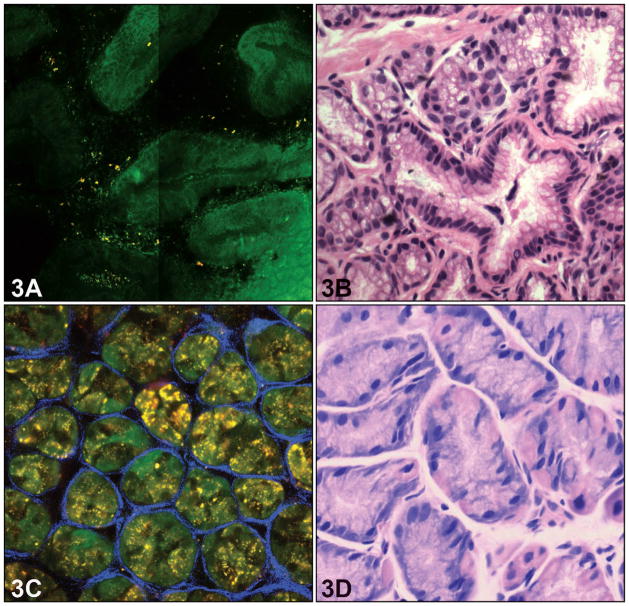
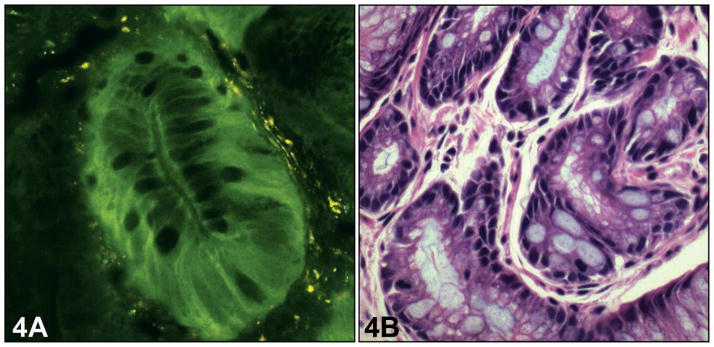
Results: Based on effective 2-photon excitation fluorescence of cellular reduced pyridine nucleotides and flavin adenine dinucleotide and lack of 2-photon excitation fluorescence of mucin and cellular nuclei, MPM could readily identify and distinguish among squamous epithelial cells, goblet cells, gastric foveolar-type mucous cells, and parietal cells in the area of gastroesophageal junction. Based on the cell types identified, the mucosa was defined as squamous, columnar gastric type (cardia/fundic-type), and metaplastic columnar intestinal-type/BE. Various types of mucosa seen in the study of 35 biopsies included normal squamous mucosa only (n = 14; 40%), gastric cardia-type mucosa only (n = 2; 6%), gastric fundic mucosa (n = 6; 17%), and both squamous and gastric mucosa (n = 13; 37%). Intestinal metaplasia was identified by the presence of goblet cells in 10 of 25 cases (40%) leading to a diagnosis of BE on MPM imaging and only in 7 cases (28%) by histopathology. In 3 of 35 biopsies (9%), clear-cut goblet cells were seen by MPM imaging but not by histopathology, even after the entire tissue block was sectioned. Based on effective 2-photon excitation fluorescence of elastin and second-harmonic generation of collagen, connective tissue in the lamina propria and the basement membrane was also visualized with MPM.
Conclusions: Multiphoton microscopy has the ability to accurately distinguish squamous epithelium and different cellular elements of the columnar mucosa obtained from biopsies around the gastroesophageal junction, including goblet cells that are important for the diagnosis of BE. Thus, use of MPM in the endoscopy suite might provide immediate microscopic images during endoscopy, improving screening and surveillance of patients with BE.
Conflict of interest statement
The authors have no relevant financial interest in the products or companies described in this article.
Figures
References
-
- Shaheen NJ, Richter JE. Barrett’s oesophagus. Lancet. 2009;373(9666):850–861. - PubMed
-
- Spechler SJ. Clinical practice: Barrett’s esophagus. New Engl J Med. 2002;346(11):836–842. - PubMed
-
- Lepage C, Rachet B, Jooste V, Faivre J, Coleman MP. Continuing rapid increase in esophageal adenocarcinoma in England and Wales. Am J Gastroenterol. 2008;103(11):2694–2699. - PubMed
-
- Pohl H, Welch HG. The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst. 2005;97(2):142–146. - PubMed
-
- Portale G, Hagen JA, Peters JH, et al. Modern 5-year survival of resectable esophageal adenocarcinoma: single institution experience with 263 patients. J Am Coll Surg. 2006;202(4):588–596. discussion 596–588. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources