

Brazilian Thalassemia Association protocol for iron chelation therapy in patients under regular transfusion
- PMID: 24478610
- PMCID: PMC3905826
- DOI: 10.5581/1516-8484.20130106
Brazilian Thalassemia Association protocol for iron chelation therapy in patients under regular transfusion
Abstract
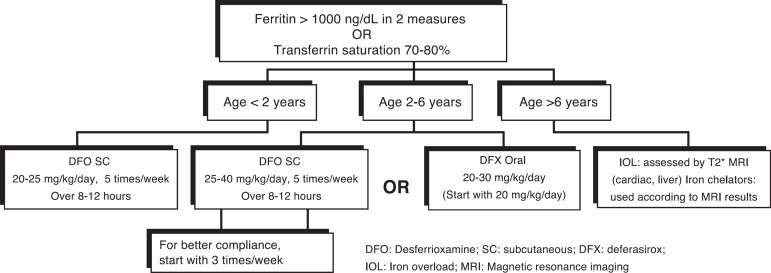
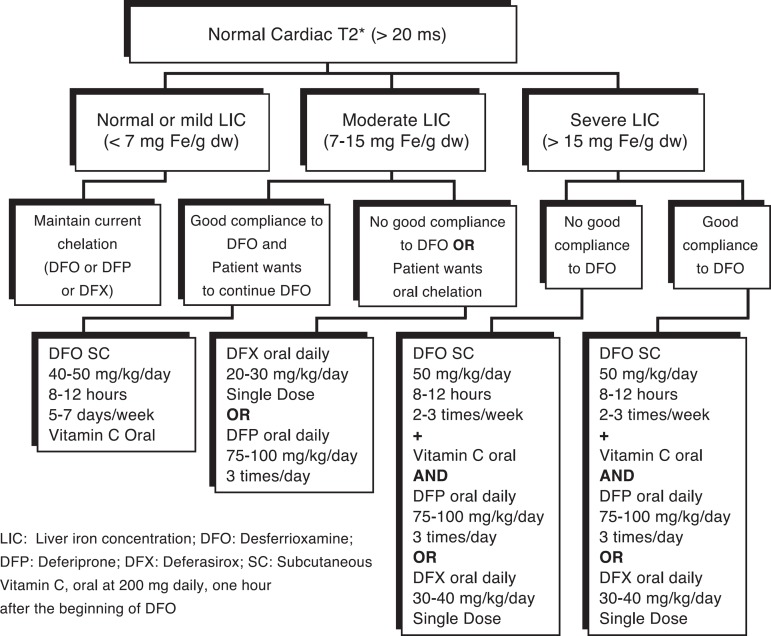
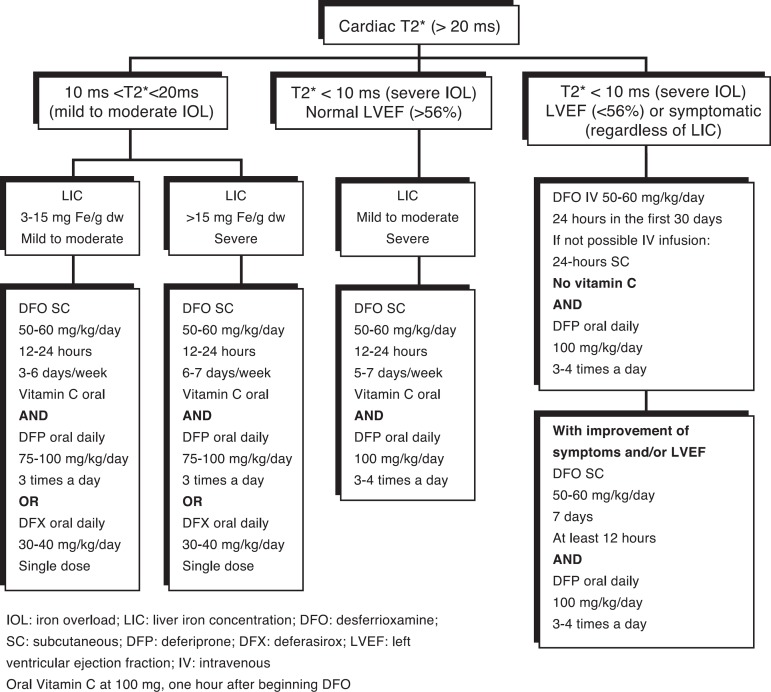
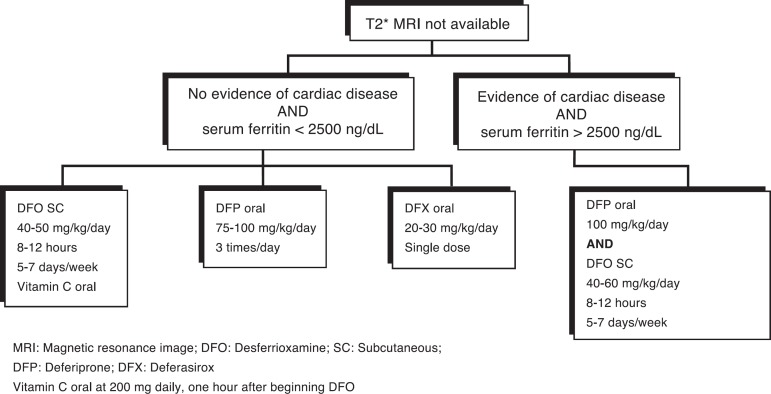
In the absence of an iron chelating agent, patients with beta-thalassemia on regular transfusions present complications of transfusion-related iron overload. Without iron chelation therapy, heart disease is the major cause of death; however, hepatic and endocrine complications also occur. Currently there are three iron chelating agents available for continuous use in patients with thalassemia on regular transfusions (desferrioxamine, deferiprone, and deferasirox) providing good results in reducing cardiac, hepatic and endocrine toxicity. These practice guidelines, prepared by the Scientific Committee of Associação Brasileira de Thalassemia (ABRASTA), presents a review of the literature regarding iron overload assessment (by imaging and laboratory exams) and the role of T2* magnetic resonance imaging (MRI) to control iron overload and iron chelation therapy, with evidence-based recommendations for each clinical situation. Based on this review, the authors propose an iron chelation protocol for patients with thalassemia under regular transfusions.
Keywords: Blood transfusion; Brazil; Chelation therapy; Deferasirox; Deferiprone; Iron chelating agents; Iron overload; Iron/metabolism; Magnetic resonance imaging; Practice guidelines as topic; Protocols; beta-Thalassemia.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interest
Figures
References
-
- Borgna-Pignatti C, Rugolotto S, De Stefano P, Zhao H, Cappellini MD, Del Vecchio GC, et al. Survival and complications in patients with thalassemia major treated with transfusion and deferoxamine. Haematologica. 2004;89(10):1187–1193. Comment in: Haematologica. 2004;89(10):1157-9. - PubMed
-
- Cunningham MJ, Macklin EA, Neufeld EJ, Cohen AR, Thalassemia Clinical Research Network Complications of beta-thalassemia major in North America. Blood. 2004;104(1):34–39. - PubMed
-
- Brittenham GM, Griffith PM, Nienhuis AW, McLaren CE, Young NS, Tucker EE, et al. Efficacy of deferoxamine in preventing complications of iron overload in patients with thalassemia major. N Engl J Med. 1994;331(9):567–573. Comment in: N Engl J Med. 1995;332(4):270-1. N Engl J Med. 1995;332(4):271-2. N Engl J Med. 1994;331(9):609-10. - PubMed
-
- Olivieri NF, Nathan DG, MacMillan JH, Wayne AS, Liu PP, McGee A, et al. Survival in medically treated patients with homozygous beta-thalassemia. N Engl J Med. 1994;331(9):574–578. Comment in: N Engl J Med. 1995;332(4):271; author reply 272-3; N Engl J Med. 1995;332(4):271-2; author reply 272-3; N Engl J Med. 1994; 331(9):609-10. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources