

Nurse and physician barriers to spiritual care provision at the end of life
- PMID: 24480531
- PMCID: PMC4569089
- DOI: 10.1016/j.jpainsymman.2013.09.020
Nurse and physician barriers to spiritual care provision at the end of life
Abstract
Context: Spiritual care (SC) from medical practitioners is infrequent at the end of life (EOL) despite national standards.
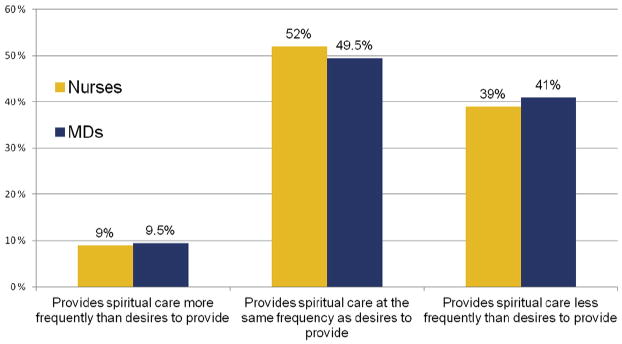
Objectives: The study aimed to describe nurses' and physicians' desire to provide SC to terminally ill patients and assess 11 potential SC barriers.
Methods: This was a survey-based, multisite study conducted from October 2008 through January 2009. All eligible oncology nurses and physicians at four Boston academic centers were approached for study participation; 339 nurses and physicians participated (response rate=63%).
Results: Most nurses and physicians desire to provide SC within the setting of terminal illness (74% vs. 60%, respectively; P=0.002); however, 40% of nurses/physicians provide SC less often than they desire. The most highly endorsed barriers were "lack of private space" for nurses and "lack of time" for physicians, but neither was associated with actual SC provision. Barriers that predicted less frequent SC for all medical professionals included inadequate training (nurses: odds ratio [OR]=0.28, 95% confidence interval [CI]=0.12-0.73, P=0.01; physicians: OR=0.49, 95% CI=0.25-0.95, P=0.04), "not my professional role" (nurses: OR=0.21, 95% CI=0.07-0.61, P=0.004; physicians: OR=0.35, 95% CI=0.17-0.72, P=0.004), and "power inequity with patient" (nurses: OR=0.33, 95% CI=0.12-0.87, P=0.03; physicians: OR=0.41, 95% CI=0.21-0.78, P=0.007). A minority of nurses and physicians (21% and 49%, P=0.003, respectively) did not desire SC training. Those less likely to desire SC training reported lower self-ratings of spirituality (nurses: OR=5.00, 95% CI=1.82-12.50, P=0.002; physicians: OR=3.33, 95% CI=1.82-5.88, P<0.001) and male gender (physicians: OR=3.03, 95% CI=1.67-5.56, P<0.001).
Conclusion: SC training is suggested to be critical to the provision of SC in accordance with national care quality standards.
Keywords: Palliative care; hidden curriculum; religion; spiritual care; spirituality.
Copyright © 2014 American Academy of Hospice and Palliative Medicine. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- World Health Organization. Palliative care: Symptom management and end of life care. [Accessed May 1, 2013];Integrated management of adolescent and adult illness. 2004 Available from http://www.who.int/hiv/pub/imai/genericpalliativecare082004.pdf.
-
- National Consensus Project. Clinical practice guidelines for quality palliative care. 2nd. Pittsburgh, PA: National Consensus Project; 2013.
-
- The Joint Commission. Spirituality, religion, beliefs, and cultural diversity. JCAHO's Standards/Elements of Performance Manual for Hospitals E-dition. 2013 PC. 02.02.13.
-
- Steinhauser KE, Christakis NA, Clipp EC, et al. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA. 2000;284:2476–2482. - PubMed
-
- Alcorn SR, Balboni MJ, Prigerson HG, et al. “If God wanted me yesterday, I wouldn't be here today”: religious and spiritual themes in patients' experiences of advanced cancer. J Palliat Med. 2010;13:581–588. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
