

Surgical and clinical confirmation of temporal bone CT findings in patients with otosclerosis with failed stapes surgery
- PMID: 24481328
- PMCID: PMC7965140
- DOI: 10.3174/ajnr.A3829
Surgical and clinical confirmation of temporal bone CT findings in patients with otosclerosis with failed stapes surgery
Abstract
Background and purpose: Prior descriptions of imaging after failed stapes procedures for otosclerosis predated currently available CT technology and/or failed to assess commonly used metallic implants. The purpose of this study was to correlate temporal bone CT findings with clinically and intraoperatively determined causes of surgical failure.
Materials and methods: All patients with otosclerosis undergoing stapedectomy between December 1999 and December 2010 were identified from a search of neurotology clinical records. Patients presenting because of failed stapes surgery and having temporal bone CT scans at the time of revision surgery or clinical evaluation were included. Imaging and clinical records were retrospectively evaluated by a medical student, radiology resident, and senior neuroradiologist. Stapes prosthesis complications and relevant anatomic CT findings were correlated to clinical and intraoperative findings.
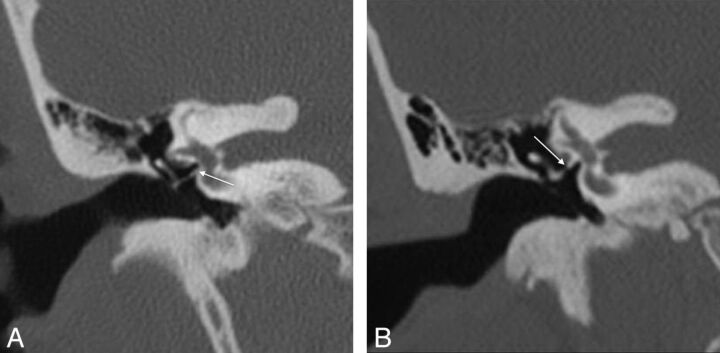
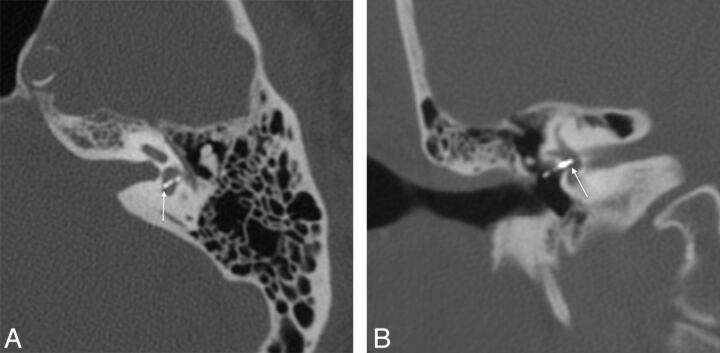
Results: Twenty-two of 340 patients met inclusion criteria. Temporal bone CT findings were correlated to intraoperative findings in 17 of 22 patients and to clinical findings in 5 of 22 patients. Surgically confirmed abnormalities included 7 of 7 incus erosions, 3 of 6 piston re-sizings, 3 of 5 granulation tissues, 3 of 5 prosthesis disconnections, 3 of 4 obliterative otosclerosis, 2 of 2 oval window dislocations, and 1 labyrinthine ossificans. Clinically confirmed abnormalities included 2 cases each of superior semicircular canal dehiscence, and wrong piston size, and 1 each of piston disconnection, labyrinthine ossificans, and intravestibular footplate.
Conclusions: CT evaluation in the setting of failed stapes surgery is challenging. Many postoperative complications such as piston migration, incus necrosis, and overt vestibular penetration are well recognized on temporal bone CT. Of particular note, superior semicircular canal dehiscence is an important contraindication to stapes surgery.
© 2014 by American Journal of Neuroradiology.
Figures








References
-
- Cummings CW, Fredrickson JM, Harker LA, et al. , eds. Otolaryngology-Head and Neck Surgery. 2nd ed. St Louis: Mosby; 1993
-
- Declau F, van Spaendonck M, Timmermans JP, et al. Prevalence of histologic otosclerosis: an unbiased temporal bone study in Caucasians. Adv Otorhinolaryngol 2007;65:6–16 - PubMed
-
- Sakihara Y, Parving A. Clinical otosclerosis, prevalence estimates and spontaneous progress. Clin Otosc Prev Acta Otol 1999;199:468–72 - PubMed
-
- Vincent R, Sperling N, Oates J, et al. Surgical findings and long-term hearing results in 3,050 stapedotomies for primary otosclerosis: a prospective study with the Otology-Neurotology Database. Otol Neurotol 2006;27(Suppl 2):S25–47 - PubMed
-
- Ozuer MZ, Olgun L, Gultekin G. Revision stapes surgery. Otolaryngol Head Neck Surg 2012;146:109–13 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous