

1,25(OH)₂D₃ induces a mineralization defect and loss of bone mineral density in genetic hypercalciuric stone-forming rats
- PMID: 24481706
- PMCID: PMC4276134
- DOI: 10.1007/s00223-014-9838-7
1,25(OH)₂D₃ induces a mineralization defect and loss of bone mineral density in genetic hypercalciuric stone-forming rats
Abstract
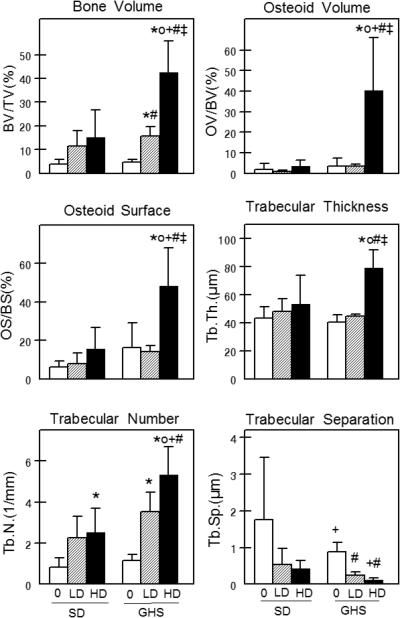
Genetic hypercalciuric stone-forming (GHS) rats, bred to maximize urine (u) calcium (Ca) excretion, demonstrate increased intestinal Ca absorption, increased bone Ca resorption, and reduced renal Ca reabsorption, all leading to elevated uCa compared to the parental Sprague-Dawley (SD) rats. GHS rats have increased numbers of vitamin D receptors (VDRs) at each site, with normal levels of 1,25(OH)₂D₃ (1,25D), suggesting their VDR is undersaturated with 1,25D. We have shown that 1,25D induces a greater increase in uCa in GHS than SD rats. To examine the effect of the increased VDR on the osseous response to 1,25D, we fed GHS and SD rats an ample Ca diet and injected either 1,25D [low dose (LD) 12.5 or high dose (HD) 25 ng/100 g body weight/day] or vehicle (veh) daily for 16 days. Femoral areal bone mineral density (aBMD, by DEXA) was decreased in GHS+LD and GHS+HD relative to GHS+veh, while there was no effect on SD. Vertebral aBMD was lower in GHS compared to SD and further decreased in GHS+HD. Both femoral and L6 vertebral volumetric BMD (by μCT) were lower in GHS and further reduced by HD. Histomorphometry indicated a decreased osteoclast number in GHS+HD compared to GHS+veh or SD+HD. In tibiae, GHS+HD trabecular thickness and number increased, with a 12-fold increase in osteoid volume but only a threefold increase in bone volume. Bone formation rate was decreased in GHS+HD relative to GHS+veh, confirming the mineralization defect. The loss of BMD and the mineralization defect in GHS rats contribute to increased hypercalciuria; if these effects persist, they would result in decreased bone strength, making these bones more fracture-prone. The enhanced effect of 1,25D in GHS rats indicates that the increased VDRs are biologically active.
Figures







References
-
- Bushinsky DA, Coe FL, Moe OW. Nephrolithiasis. In: Brenner BM, editor. The Kidney. W.B. Saunders; Philadelphia: 2012. pp. 1455–1507.
-
- Moe OW, Bonny O. Genetic Hypercalciuria. Journal of the American Society of Nephrology. 2005;16:729–745. - PubMed
-
- Stechman MJ, Loh NY, Thakker RV. Genetics of hypercalciuric nephrolithiasis: renal stone disease. Ann NY Acad Sci. 2007;1116:461–484. - PubMed
-
- Bushinsky DA, Asplin JR, Grynpas MD, Evan AP, Parker WR, Alexander KM, Coe FL. Calcium oxalate stone formation in genetic hypercalciuric stone-forming rats. Kidney Int. 2002;61:975–987. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
